

Abstrakt
Məqsəd: Mərkəzlərimizdə aparılan perikardiosintez protokolunun etibarlılıq və effektivliyinin dəyərləndirilməsi Xəstə və üsullar: Perikardial maye diaqnozu ilə 2005 oktyabr və 2009 noyabr tarixləri arasında xəstəxanaya gələn xəstələr tədqiqata daxil edildi. Ən az 1.5 sm ölçüsündə dairə şəkilli perikard mayesinin varlığı , klinik və ya exokardioqrafik tamponada əlamətləri tədqiqata daxil edilmə kriteriyaları olaraq müəyyənləşdirildi. 6 Frenç qalınlığında dilatator ilə uzun müddətli drenaj ilə icra edilən perikardiosintez proseduru etibarlılıq və effektivlik baxımından dəyərləndirildi. Nəticələr: Topamda 61 xəstə tədqiqata daxil edildi. Aparılan müalicəvi üsulun xəstələrin tamamında uğurlu nəticələndiyə gözləndi. Iki xəstədə (3.2%) yenidən perikardial maye yığılması səbəbi ilə bir prosedura daha ehtiyac oldu. Tədqiqata daxil edilən xəstələrdə ən çox qoyulan diaqnoz vərəm ( 65%) və onkoloji xəstəliklər idi (16%). Yеkun: Bu üsulun etibarlılır və effektivlik dəyərinin yüksək olması ilə yanaşı ağırlaşma riskinin azlığı və təkrar proseduraya ehtiyacın az olması aydınlaşdı.
Əsas mətn
Pericardiocentesis performed either using percutaneous or surgical approach is a well-established treatment of pericardial tamponade and massive pericardial effusions. Establishment of etiologic diagnosis in patients with pericardial effusion is another aim of pe-ricardiocentesis (1). Although surgical approach (2, 3) is preferred in patients with small amount of pericardial effusion, it is also affected by operator experience in percutaneous techniques. Advantage of surgical approach is possibility of removing of small, and localized pericardial effusions. Percutaneous pericardiocentesis method was applied effectively since 1840 (4), although it may lead to serious complications such as death, cardiac arrest, cardiac perforations, cardiac arrhythmias, arterial bleeding, pneumothorax, infection, and vagal reaction (5, 6).
Pericardiocentesis under two-dimensional echocardiographic guidance is safer and easier rather than blind approach. Two-dimensional contrast echocardiography is helpful in locating needle position; thereby significant complications can be precluded (7, 8). Prolonged drainage of pericardial fluid is generally performed to avoid reaccumulation of pericardial fluid.
Herein we report treatment and complication rates of 61 cases of pericardial effusions with different etiologies, treated by percutaneous echocardiographically guided pericardiocentesis without prolonged pericardial drainage, and describe our technique.
Patients and Methods
Patient Selection
Patients with pericardial effusion, which were admitted to hospital during the period from July 2005 through February 2009 were enrolled. Study was approved by the ethical board. Enrollment criteria included presence of at least 1.5 cm of circumferential pericardial effusion or combination of clinical and echocardiographic signs of cardiac tamponade. Diagnosis of cardiac tamponade was established based on combination of several clinical and echocardiographic findings in the presence of pericardial effusion. Moderate to severe dyspnea, orthopnea, decrease in systolic blood pressure, decrease in urine output, elevated central venous pressure and presence of pulsus paradoxus were considered as clinical signs of cardiac tamponade. Right atrial diastolic collapse, right ventricular collapse, more than 25% decrease in transmitral E wave amplitude on inspiration and failure to decrease proximal diameter of inferior vena cava on deep inspiration were considered as echocardiographic signs of cardiac tamponade. Patients who developed pericardial effusion due to trauma, thoracic surgery and patients who had coagulation abnormality, thrombocytopenia (<100 000), and those anticoagulated with warfarin were excluded from the study. The procedure was not performed in patients with suspected aortic dissection, until exclusion of this condition was performed with appropriate diagnostic imaging tools. Informed consent was obtained from all patients before the procedure. Complete blood count and coagulation parameters were assessed and general physical examination was performed before the procedure.
Description of the technique
Pericardiocentesis was performed in the coronary care unit setting, under continuous ECG (electrocardiogram), pulse oxymetry and blood pressure monitoring.
Echocardiographic evaluation: Complete two-dimensional and Doppler echocardiographic evaluation was performed before the procedure. During echocardiographic study it was aimed to evaluate location and size of effusion, presence or absence of echocardiographic signs of tamponade, to determine the presence of loculation, to evaluate stranding, and to determine the optimal site of puncture (subxiphoidal or apical). Other important information, obtained during echocardiographic examination was measurement of distance from parietal pericardium to the optimal site of puncture (measured on 2-D echocardiography device monitor as a distance from the apex of triangle to the pericardium). This distance was measured in near sitting position at 45-60° angle in which procedure was planned to be performed for patients considered to undergo a subxiphoidal approach and in semi-left decubitus position for those considered for intervention from apical approach.
In cases requiring echocardiographic guidance during the procedure, assisting operator placed the probe into the sterile glove filled with ultrasonic transmission gel and surface of skin was cleaned with povidone-iodine solution to allow the transition of ultrasonic waves.
Before procedure two routes of intravenous access on both arms were obtained. 500 ml of 0.9% NaCl solution was infused over the period of 15 minutes before procedure, and was continued to up for 1000 ml during and following the procedure.
Following a sterile preparation and draping of procedure field, approximate area of puncture was infiltrated with 20 ml of 2% prilocaine (400 mg). Puncture was performed with 18-gauge needle (5-8 cm length) under continuous negative aspiration, until the approximate distance from skin to parietal pericardium measured by echocardiography was exceeded by 1 cm. In this situation approximate direction of needle was reevaluated by echocardiography, and puncture was performed in another appropriate direction. After entering the pericardial space, a small amount of fluid (50 ml) was aspirated into the syringe and stored for further diagnostic work up. Then the syringe was removed, and 0.038-inch J-tipped guide wire (length 45.5 cm) was advanced through the needle. Once the guide wire had been advanced safely into the pericardial space, the needle was removed and dilator of 6F sheath (Input Introducer Sheath, Medtronic, Minneapolis, USA), which length is 17 cm, was advanced into the pericardial space and the guide wire was removed thereafter. Sheath was not advanced into the pericardial space, and was not used by any means during the procedure. Once the dilator was completely introduced into the pericardial space over-the-wire, fluid was aspirated until it stopped to flow into the syringe. Then the catheter was slightly withdrawn, aspiration continued at each point until it was not possible to aspirate at that position. This procedure was repeated continuously, until the dilator catheter was completely withdrawn from the pericardial space. During pericardiocentesis procedure, we aimed to remove pericardial fluid as completely as it was possible. Echocardiographic assessment was repeated before complete withdrawal of dilator from pericardial space. In patients with significant amount of residual pericardial fluid (> 1 cm), guide wire was advanced into pericardial space, dilator was further readvanced and residual fluid was aspirated. After removal of catheter, puncture site was covered with sterile closure band. In cases with hemorrhagic pericardial effusion and in those with clinical suspicion or history of underlying tuberculosis, antituberculosis treatment was started immediately, and continued until the diagnosis of tuberculosis was excluded. We believe that this approach may result in decrease of re-accumulation of pericardial fluid in subgroup of patients with underlying tuberculosis.
Echocardiographic evaluation was performed several hours (3-6) after initial procedure and repeated every day during hospitalization. Final evaluation was performed on the day of discharge from the hospital.
Results
Patient Characteristics
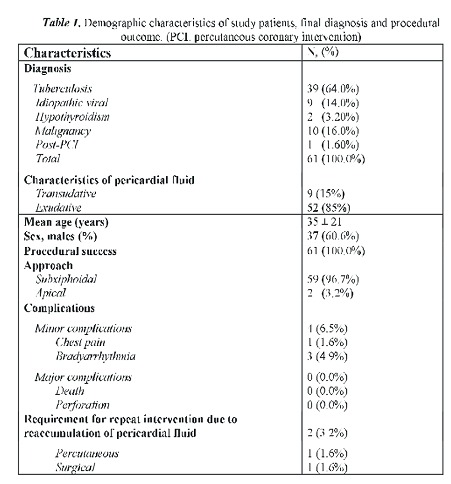
61 patients were enrolled in to the study. Data of the patients, including demographic characteristics and final diagnosis established at the time of the procedure or during subsequent diagnostic work-up is presented in Table 1.
Procedure related complications and outcome
Procedure was successfully performed in all patients. There were no major complications, such as death, hemodynamic compromise, or requirement for urgent cardiothoracic surgery during the procedure or subsequent follow-up.
Procedure was performed via subxiphoidal approach in 59 patients and via apical approach in 2 patients. We observed only four minor complications, such as severe chest pain in one patient and severe bradycardia responsive to administration of atropine in three patients. Chest pain was suggested to be a consequence of irritation of intercostal nerves during an apical approach and bradycardia due to either insufficient local anesthesia or irritation of the vagal fibers of diaphragm, pericardium or right ventricular wall. Re-accumulation of pericardial fluid within pericardial space, requiring second intervention was observed in two patients: one with hypothyroidism and one during serous stage of pericarditis secondary to tuberculosis. Accumulation of pericardial fluid within left pleural space was observed in 7 patients, which was suggested to be secondary to the formation of connection between pericardial and pleural spaces. Two of these patients had undergone apical and five of them subxiphoidal approach, and pericardial effusion had serous character in all of these patients. None of the patients with hemorrhagic effusion had transition of fluid in to the pleural space. These cases were successfully managed without need for left-sided thoracentesis. This fluid disappeared during the follow-up in all patients.
Another important observation was made in one patient who developed pericardial effusion after percutaneous coronary intervention (PCI). This patient was managed with pericardiocentesis and intrapericardial administration of tranexamic acid, which resulted in rapid cessation of hemorrhage. We suggest that this finding needs further investigation in patients with post-PCI pericardial effusion, because local administration of antifibrinolytic agents may help to avoid thrombotic complication when compared to administration of these agents into the central circulation.
Echocardiographic measurement of distance between skin and pericardial fluid at puncture site, was found to be highly correlated with needle depth required to achieve pericardial space (r=0.953, p<0.0001). This measurement may help to avoid traumatic complications associated with pericardiocentesis procedure.
Total volume of pericardial fluid aspirated in this study cohort was 1370 ± 920 ml (250 - 2700 ml).
Discussion
Pericardiocentesis via the subxiphoidal approach was reported as a safest method to avoid procedure related complications (9). Two-dimensional echocardiography helps to improve procedural outcome via the perception of spatial orientation, while pericardial contrast injection provides optimal identification of the needle tip (8, 10, 11). Morbidity and mortality rates with blind pericardiocentesis via subxiphoidal approach, was reported as high as 50% and 6%, respectively. Otherwise, echo-guided pericardiocentesis was associated with fewer complication rates (12-14).
First of all, technique of pericardiocentesis presented here is very cost effective and safe irrespective of underlying disease. Cost of procedural equipment is about 10 US dollars, and this price is significantly lower when compared to use of specially designed catheters for peri-cardiocentesis or standard angiographic pigtail catheters. Although, Tsang et al. was reported that extended catheter drainage in patients who underwent echo-guided pericardicentesis, offered decrease in recurrence (14), based on our observation we suggest that extended drainage of pericardial fluid is not necessary in significant proportion of patients. Although, it is well known that patients with tuberculosis pericarditis and those who have serous effusions secondary to hypothyroidism or hypoalbuminemia have higher effusion recurrence rates, in our opinion initiation of antituberculosis treatment immediately after the procedure in all patients with suspicion of this disease, may decrease fluid reaccumulation rates and need for long-term pericardial drainage. However this hypothesis needs further prospective investigation.
We preferred use of dilator instead of sheath, because of several reasons: distal edge of sheath may result in myocardial damage, and sheaths are prone to kinking within pericardial space. However dilator is much more stiff than sheath and is not prone to kinking. It can be speculated that its distal edge may also result in myocardial damage, but we have noted in methods section that dilator was only withdrawn and in case of need for further readvancement dilator was advanced over the guide wire.
Another important finding of this study, is observation of correlation between real and echocardiographically measured distance from skin to pericardium. This approach may help to reduce procedure related traumatic complications. In addition we and other investigators recommend that the puncture site of pericardiocentesis should be determined with two-dimensional echocardiography (15). Absence of major complications, only three minor complications in this study, may be explained by operator experience, however we suggest that technique described here is very safe and effective even in inexperienced hands. Selection of either apical or subxciphoidal approach depends on the location of pericardial fluid. And we suggest that puncturing the site where pericardial effusion leads to increase between parietal and visceral pericardium, may help to decrease procedure related major complications.
Low rate of re-accumulation of pericardial effusion depends on several factors. First of all, significant proportion of patients enrolled in the study had hemorrhagic pericardial effusion, with excessive stranding, and we suggest that, complete removal of fluid results in adhesion between visceral and parietal pericardium, and by this way prevents re-accumulation of pericardial fluid. Second factor, is very high rate of tuberculous pericarditis. Also need for repeated pericardiocentesis is high for patients with tuberculosis; we routinely start empirical treatment with antituberculosis agents in all patients with hemorrhagic pericardial effusion and as it was mentioned before this issue may explain low incidence of fluid reaccumulation in our cohort. Although, hemorrhagic pericardial effusions due to tuberculosis are uncommon in developed countries (16), in our country the incidence of tuberculosis and tuberculosis pericardial effusions is higher and similar to African and Asian countries (17, 18).
Another important factor is formation of pleuro-pericardial connections after removal of catheter, which results in flow of pericardial fluid to pleural space. All patients who had developed left sided pleural effusion following pericardiocentesis, had serous effusions and were managed without need for thoracentesis. It is not surprising that none of these patients had hemorrhagic effusions and we suggest that fibrin strands prevent formation of pleuro-pe-ricardial connections in patients with hemorrhagic effusions. Increased pleural capability of fluid absorption obviates need for further interventional procedures such as thoracentesis.
One of the important points that we would like to mention here is periprocedural bradyar-rhythmia, which can sometimes be disastrous complication. This may be prevented by sufficient local anesthesia. Inexperienced operators, prefer to abort procedure and initiate resuscitation in cases of periprocedural bradyarrhythmias/hypotension as a consequence of vasovagal reaction. However, we strongly recommend continuing procedure with simultaneous administration of atropine, fluid and vasodepressors when necessary, and especially in patients with cardiac tamponade and massive pericardial effusion. This argument is based on the fact, that cardiopulmonary resuscitation is not effective in restoration of circulation in the setting of cardiac tamponade (19). Rapid pericardiocenthesis, with even very small amount (20-50 ml) of fluid removal is life saving in this setting, because of the very high mortality associated with cardiac tamponade and cardiac arrest (1, 20, 21). We routinely administer a large amount of intravenous fluid before and during the procedure as described in methods section, and this helps to support filling pressures, even during severe bradyarrhythmias. In addition, intravenous fluid administration may prevent 'decompressive syndrome', which may be seen after removing of large amount (>500 ml) of pericardial fluid (21). Although, cases of acute pulmonary congestion and acute transient left ventricular systolic failure after large volume pericardiocentesis have been reported (22), we did not observed this kind of complication in our patients. Thus, we strictly advise pre- and perioperative administration of intravenous fluid without concomitant treatment with vasopressor agents to avoid hemodynamic compromise.
Conclusion
Here we presented very simple, effective and safe technique of pericardiocentesis. Although we understand that this issue needs further prospective evaluation, we suggest that early administration of antituberculosis treatment in countries with high incidence of this disease seems to be an effective approach toward decreasing the rate of fluid reaccumulation.
Şəkillər
Açar sözlər
İstinadlar
- Cooper JP, Oliver RM, Currie P, Walker JM, Swanton FH. How do the clinical findings in patients with pericardial effusions influence the success of aspiration? Br Heart J 1995; 73: 351-354.
- Levin BH, Aaron BL. The subxiphoid pericardial window. Surg Gynecol Obstet 1982; 155: 804-806.
- Alcan KE, Zabetakis PM, Marino ND, Franzone AJ, Michelis MF, Bruno MS. Management of acute cardiac tamponade by subxiphoid pericardiotomy. JAMA. 1982; 247: 1143-1148.
- Kilpatrick ZM, Chapman CB. On pericardiocentesis. Am J Cardiol 1965; 16: 722-728.
- Wong B, Murphy J, Chang CJ, Hassenein K, Dunn M. The risk of pericardiocentesis. Am J Cardiol 1979; 44: 1110-1114.
- Duvernoy O, Borowiec J, Helmius G, Erikson U. Complications of percutaneous pericardiocentesis under fluorocoscopic guidance. Acta Radiol. 1992; 33: 309-313.
- Chandraratna PA, Reid CL, Nimalasuriya A, Kawanishi D, Rahimtoola SH. Application of 2-dimensional contrast studies during pericardiocentesis. Am J Cardiol 1983; 52: 1120-1122.
- Callahan JA, Seward JB, Tajik AJ. Cardiac tamponade: pericardiocentesis directed by two-dimensional echocardiography. Mayo Clin Proc. 1985; 60:344-347.
- Marfan A B. Ponction du pericarde par l'ep'gastre. Ann de Med et chir inf. 1911; 15:529-531.
- Martin RP, Rakowski H, French J, Popp RL. Evaluation of pericardial effusion with wide angle phased-array echocardiography. Am J Cardiol 1978; 42: 904- 912.
- Vayre F, Lardoux H, Pezzano M, Bourdarias JP, Dubourg O. Subxiphoid pericardiocentesis guided by contrast two-dimensional echocardiography in cardiac tamponade: experience of 110 consecutive patients. ur J Echocardiography 2000; 1: 66-71.
- Krikorian JG, Hancock EW. Pericardiocentesis. Am J Med 1978; 65: 808-814.
- Moores DW, Dziuban SW Jr. Pericardial drainage procedures. Chest Surg Clin North Am 1995; 5: 359- 373.
- Tsang TS, Barnes ME, Hayes SN, Freeman WK, Dearani JA, Butler SL, et al. Clinical and echocardiographic characteristics of significant pericardial effusions following cardiothoracic surgery and outcomes of echo-guided pericardiocentesis for management. Mayo Clinic Experince 1979-1998. Chest 1999; 116: 322-331.
- Kim SW, Hwang SO, Lee KH, Cho JH, Kang KH, Moon JB, et al. Is a Subcostal Approach Always Suitable for Emergency Pericardiocentesis?. J Korean Soc Emerg Med 2000; 11: 331-338.
- Atar S, Chiu J, Forrester JS, Siegel RJ. Is the Cause Cancerous, Tuberculous, or Iatrogenic in the 1990s? Chest 1999; 116:1564 -1569.
- Desai HN. Tuberculous pericarditis. A review of 100 cases. S Afr Med J 1979;55:877-80.
- Jain S, Sharma N, Varma S, Rajwanshi A, Verma JS, Sharma BK. Profile of cardiac tamponade in the medical emergency ward of a North Indian hospital. Can J Cardiol 1999;15:671-5.
- Anthi A, Tzelepis GE, Alivizatos P, Michalis A, Palatianos GM, Geroulanos S. Unexpected cardiac arrest after cardiac surgery: incidence, predisposing causes, and outcome of open chest cardiopulmonary resuscitation. Chest 1998;113: 15-19.
- Ceron L, Manzato M, Mazzaro F, Bellavere F. A new diagnostic and therapeutic approach to pericardial effusion. Chest 2003; 123: 1753-1758.
- Collins D. Aetiology and management of acute cardiac tamponade. Crit Care Resusc 2004; 6: 54-58.
- Chamoun A, Cenz R, Mager A, Rahman A, Champion C, Ahmad M, et al. Acute left ventricular failure after large volume pericardiocentesis. Clin Cardiol 2003; 26: 588-590.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 10.Apr.2012
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 2057