

Abstrakt
Müqavimətli hipertenziya, xəstə 3 antihipertenziv dərmanın müvafiq kombinasiyasının tam dozasını istifadə etdikdə, hədəf qan təzyiqinə (ümumi hipertansif əhalidə <140/90 mm Hg və diabet və ya XBH olan xəstələrdə <130/80 mm Hg) nail olunmaması kimi müəyyən edilir. dərmanlar, o cümlədən diüretik. Müqavimətli hipertansiyonun dəqiq yayılması və tezliyi məlum olmasa da, əhali tədqiqatlarından və klinik sınaqlardan əldə edilən dolayı sübutlar bunun ümumi bir klinik problem olduğunu göstərir. Həqiqi rezistent hipertenziyanı təsdiqləmək üçün ağ xalat effekti, suboptimal qan təzyiqi ölçmə texnikası və təyin edilmiş dərmanlara zəif riayət edilməsi ilə bağlı psevdorrezistentliyi istisna etmək lazımdır. Müalicənin ilk addımı həyat tərzi və pəhriz modifikasiyası, müqavimətə səbəb olan dərmanların aradan qaldırılması və hipertoniyanın potensial ikincili səbəblərini qiymətləndirməkdir. Farmakoloji müalicə xəstənin klinik xüsusiyyətlərinə uyğunlaşdırılmalı və müqavimətin məsul yoluna yönəldilməlidir. Optimal terapiya almasına baxmayaraq, nəzarətsiz hipertenziyası olan xəstələr böyrək denervasiyası və karotid baroreseptorların stimullaşdırılması kimi yeni müdaxilə müalicələrinə namizəddirlər.
Əsas mətn
Introduction
Resistant hypertension (RH) is an important clinical problem that both primary care physicians and specialists encounter in daily practice. RH is defined classically as a therapeutic strategy which includes appropriate lifestyle measures plus a diuretic and two other antihypertensive drugs belonging to different classes at adequate doses (but not necessarily including a mineralocorticoid receptor antagonist) fails to lower systolic blood pressure (SBP) and diastolic blood pressure (DBP) values below 140 and 90 mmHg , respectively in general population [1] Another definition subsequently proposed that patients requiring ≥4 drugs irrespective of their blood pressure (BP) values are classified as RH [2].
RH is associated with great cardiovascular and renal risks such as heart failure, chronic kidney disease (CKD), hypertensive heart disease, stroke as well as cardiac arrhythmias and it became more popular with novel nonpharmacological methods such as renal denervation and carotid baroreceptor stimulation [3].
This review provides an overview of the clinical features, diagnosis, conventional and novel pharmacological therapies and the invasive nonpharmacological approaches of RH.
Prevalence and Incidence
Epidemiology of RH is related to the characteristics of the population under examination and intensity of the treatment. The prevalence of RH has been reported to range from 5-30% of the overall hypertensive population but probably the real prevalence is less than 10% [4-7][8]
Data from a national registry of ambulatory BP monitoring, prevalence of RH was found as 14% [5] however in the NHANES III 8.9% of all adult hypertensives and 12.8% of the treated hypertensives fulfilled the criteria for RH [7]. Patients with CKD tend to have RH. The prevalence of RH in this group is 15.8%, 24.9%, and 33.4% for those with estimated glomerular filtration rate (eGFR) ≥60, 45–59, and <45 mL/min per 1.73 m2, respectively, and 12.1%, 20.8%, 27.7%, and 48.3% for albumin-to-creatinine ratio <10, 10–29, 30–299, and ≥300 mg/g, respectively [9].
There is a large number of prevalence studies, however only one about incidence. Daugherty and coworkers [6] studied the incidence of RH among 205,750 hypertensive patients who initiated antihypertensive treatment between 2002 and 2006. Excluding patients with pseudoresistance, the incidence of RH was 0.7 per 100 patients/year.
It is obvious that, RH will become increasingly common, driven by an aging population, obesity and nonadherence trends.
Prognosis
The prognosis of RH is unknown, but cardiovascular risk increases if patient’s history of hypertension is long-standing, severe hypertension is complicated by multiple cardiovascular (CV) risk factors such as diabetes, obesity, CKD, and sleep apnea.Patients with RH are more likely to have target organ damage and a higher long-term CV risk than patients whose BP is under control.Heart failure, myocardial infarction, renal failure and stroke are in concordance with the level of BP elevation [10].
Daugherty et al. analyzed longitudinal data of a 5-year period and demonstrated a 50% increase in CV events, largely attributable to the development of CKD in patients with RH compared to patients who had controlled BP [6].
It is unknown how much CV risk is reduced by antihypertensive treatment. The benefits of successful treatment, however, are likely substantial as suggested by hypertension outcome studies in general. How much of this benefit occurs with successful treatment of RH is unknown [10].
Diagnosis and Evaluation
RH can be real or spurious and it has multiple and various causes. Therefore, it is essential to follow some steps to be sure that the patient has RH. A frequent cause of spurious RH is not to adhere to the treatment plan. Lack of BP control may, however, also depend on following issues:
1) Persistence of an alerting reaction to the BP-measuring procedure, with an elevation of office (although not of out-of-office) BP (white coat hypertension)
2) Use of small cuffs on large arms, with inadequate compression of the vessel
3) Pseudohypertension (Table 1) [11]
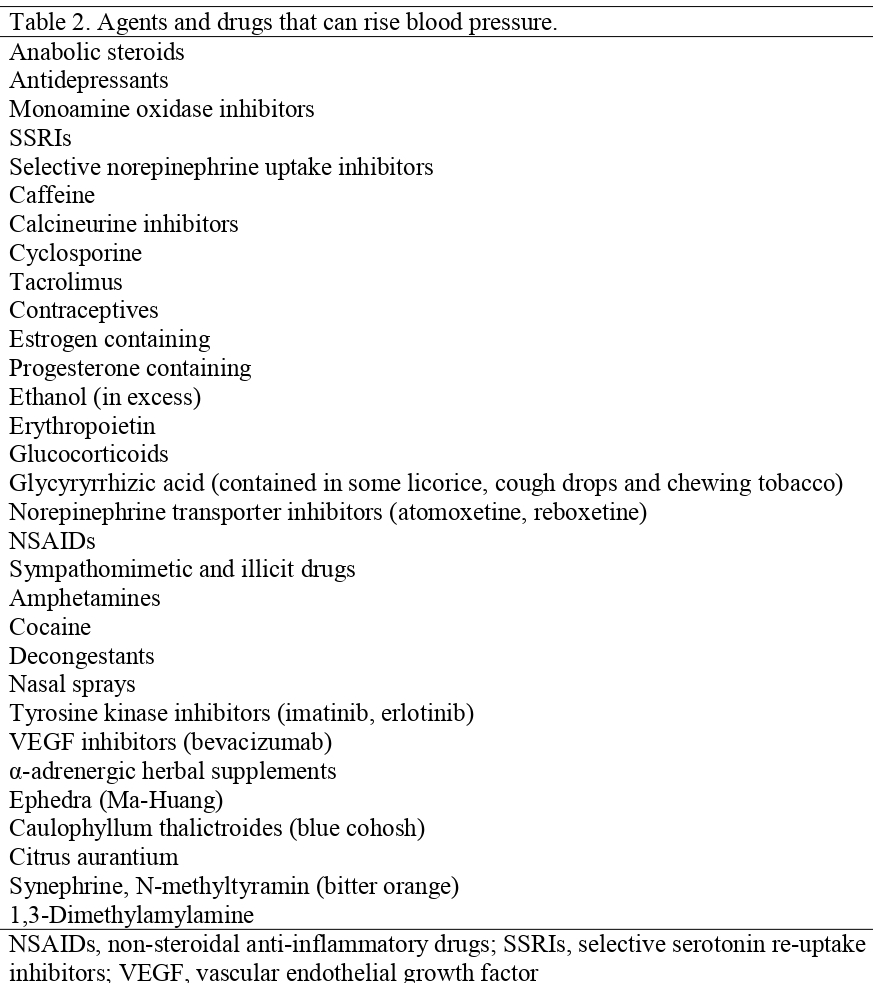
True resistant hypertension may originate from following reasons (Table 2 and 3):
1) Lifestyle factors such as obesity or large weight gains, excessive alcohol consumption, high salt intake
2) Chronic intake of vasopressor or sodium-retaining substances
3) Obstructive sleep apnea (OSA)
4) Undetected secondary forms of hypertension
5) Advanced and irreversible organ damage, particularly when it involves renal function or leads to a marked increase in arteriolar wall-lumen ratio or reduction of large artery distensibility [1].
To exclude white-coat hypertension; out-of-office BP measurements, 24-hour ambulatory BP monitoring or home BP is recommended. It is also shown that out-of-office BP measurements give better prognostic information [12-15].
Another possible cause of spurious elevated BP is false BP measurement technique. If the patient is not allowed to rest or if an inappropriately small cuff is used, BP may be falsely elevated. Patients should be allowed to rest for at least 5 minutes with their back supported and arm at heart level prior to measurement.Using an inappropriately smaller cuff may result in elevations of SBP readings from 5 to 15 mmHg. Smoking can also elevate SBP; therefore, patients should be asked about tobacco use [16-18].
Pseudohypertension is a result of marked arterial stiffening (more common in the elderly, especially with heavily calcified arteries) which prevents occlusion of the brachial artery.
After exclusion of spurious reasons listed above; a second and more difficult step is to exclude low adherence to pharmacologic regimen in RH.
Diagnosis of RH is based on BP elevation despite adherence to a regimen of 3 medications at full doses. Treatment adherence is crucial in blood pressure control, and monitoring patient adherence is essential to the successful management of hypertension, since nonadherence is associated with poor prognosis [19, 20]. Potential side effects, cost of medication, and complex regimens are some possible causes of nonadherence [16].
There are some ways to assess whether patients take their medication as recommended or not. These include interviewing with the patient, pill counting, prescription follow-up, assays of drugs in blood or urine, and the use of electronic pill dispensers but these techniques are not easy to apply because they are not reliable, easy-to-use and economical [21].
Lifestyle factors such as obesity or large weight gains, excessive alcohol consumption, and high sodium intake, may oppose the BP-lowering effect of antihypertensive drugs.
Several classes of pharmacological agents can produce transient or persistent increases in BP [22]. NSAIDs are a common cause of RH, may increase BP by an average of 5 mmHg through sodium and fluid retention [23]. They interfere with all antihypertensive agents except calcium antagonists. Selective cyclo-oxygenase-2 inhibitors have effects similar to those of NSAIDs [24]. Sympathomimetic agents (anorectic pills, nasal decongestants, amphetamine-like stimulants, cocaine), oral contraceptives, anabolic steroids, glucocorticoids, erythropoietin, and cyclosporine are also commonly used agents that can interfere with BP control [10, 20]. Illicit drugs, such as cocaine, also can be a cause of RH.
OSA is common among RH patients, especially if they are obese. OSA causes RH because nocturnal hypoxia, chemoreceptor stimulation, and sleep deprivation may have a long-lasting vasoconstrictor effect. A definitive diagnosis requires a sleep laboratory study. Treatment with a continuous positive airway pressure (CPAP) device has been shown to reduce BP and found to be beneficial in RH with OSA [10].
Patients with RH are much more likely to have an identifiable cause of hypertension (secondary hypertension). Previous studies have shown that 5-10% of RH has an identifiable cause [25, 26]. Renal parenchymal disease, as the most common medical cause of secondary hypertension, must be considered [20, 27]. Renal arterial disease, OSA, primary hyperaldosteronism, pheochromocytoma, Cushing’s syndrome, hyper- and hypoparathyroidism, aortic coarctation and intracranial tumors are other causes of secondary hypertension and requires evaluation by a specialist.
Treatment
In any case, treatment should be tailored to the patient's profile, lifestyle, and comorbidities. Only such kind of management would be well tolerated and maintain long-term compliance.
Nonpharmacologic Treatment
Reduction of sodium intake and CPAP therapy have demonstrated efficacy in reducing BP of RH in subjects with OSA [21]. Besides, weight reduction in overweight/obese subjects, alcohol restriction, smoking cessation, regular physical exercise can provide additional benefits for BP control [1, 21].
Pharmacologic Management of Resistant Hypertension
Pharmacological treatment should be based on the most common causes of RH and focused on blocking all the physiological pathways.
Antihypertensive agent doses should be titrated upward until BP is controlled or the maximum recommended dosage is reached, unless the patient experiences dose related adverse effects. It is then appropriate to add a drug from another class that has additive or synergistic effects with the first drug. In general, a typical regimen should include a diuretic, an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB), a calcium channel blocker (CCB), and a beta-blocker (unless these drugs are contraindicated or not tolerated, or other drugs are indicated due to comorbidities).
Special attention has to be drawn in maximizing the dose of diuretics or switching to loop diuretics in patients with low GFR. The overactivation of the sympathetic nervous system renders beta-blockers, alpha blockers, and centrally acting antihypertensive drugs (clonidine, alpha methyldopa etc.) of potential benefit in many patients when added in previous therapy. Direct vasodilators (hydralazine and minoxidil) can be very effective in BP management, especially in patients with CKD.
Plasma aldosterone and aldosterone-to-renin ratio is reported higher in patients with resistant hypertension compared with subjects with controlled blood pressure [28]. A number of non-randomised trials have shown the effectiveness of low dose spironolactone on lowering blood pressure in patients with resistant hypertension [28-33]. Moreover, Nishizaka et al. reported that low dose spironolactone decreased blood pressure by 21/10 mmHg in 3 weeks and 25/12 mmHg at 6 months in patients with resistant hypertension with and without primary hyperaldosteronism [29]. In another study low dose spironolactone decreased blood pressure in patients with resistant hypertension by 26/11 mmHg at 6 months after starting the drug [32]. The most robust, double-blind, placebo controlled crossover study, PATHWAY-2, examined the effect of spironolactone (in a dose of 25–50 mg) versus placebo, bisoprolol (in a dose of 5–10 mg), and doxazosin (in a dose of 4–8 mg) in resistant hypertension. Spironolactone provided the most effective and reduced blood pressure decline by 10 mmHg, more than placebo, by 5- 6 mmHg more than doxazosin and bisoprolol, and doxazosin alone and bisoprolol alone. The decline of home systolic BP after 12 weeks was 14.4mmHg. The average decline was 13/6 mmHg for home BP and 21/ 10 mmHg for office BP. Spironolactone led to the achievement of target home BP values in 58 % of the patients [34]. The efficacy and safety of spironolactone was examined in resistant hypertensive patients with chronic kidney disease. The study of Verdalles et al. compared spironolactone addition (in a dose of 25 mg) to loop diuretic (furosemide in a dose of 40 mg) in 30 patients with resistant hypertension. Most of the patients were previously treated with thiazide and were diagnosed with chronic kidney disease with mild kidney failure (estimated glomerular filtration was <60 mL/min in 60% of patients). At 6 months, office BP decreased by 24/11 mmHg in the spironolactone group, compared with 14/5 mmHg in the furosemide group. Two cases of hyperkalemia were recorded in the spironolactone group [35].
Oliveras et al. compared blood pressure decreasing effect of spironolactone with renal sympathetic denervation to treat true resistant hypertension in a randomized clinical trial. Spironolactone provided more effective reducing 24-h SBP and 24-h DBP: mean baseline-adjusted differences between the two groups were −17.9 mm Hg (95%CI −30.9 to −4.9); P = 0.010 and −6.6 mmHg (95%CI −12.9 to −0.3); P = 0.041, for 24-h SBP and 24-h DBP, respectively. As regards changes in office blood pressure, mean baseline-adjusted differences between the two groups were −12.1 mmHg (95%CI −29.1 to 5.1); P = 0.158 and of −5.3 mmHg (95%CI −16.3 to 5.8); P = 0.332, for office SBP and office DBP, respectively [36].
Other randomized controlled trials have also shown the efficacy of spironolactone in patients with drug resistant hypertension [37-42].
Chronotherapy is shown to be beneficial in RH such as administration of one antihypertensive drug at bedtime has been shown to improve BP control [43-45].
Polypharmacy is difficult to avoid in clinical practice. In the long run, most of these patients require more doses and classes of drugs. Fixed dose combinations offer the convenience of taking fewer pills, combining antihypertensive agents with additive or synergistic effect and reducing dose-dependent adverse effects of individual components.
Novel drugs for the management of Resistant Hypertension
Novel drugs are also being investigated such as endothelin receptor antagonists (ERAs). ERAs exhibited promising results in preliminary studies about management of RH [46].
The DORADO trial recently evaluated the efficacy and safety profile of the selective endothelin receptor blocker darusentan in patients treated with more than four antihypertensive drugs (including a diuretic) but without effective blood pressure control. The trial results show that > 50% of patients treated with the drug exhibit clinical blood pressure < 140/90 mmHg and well-controlled ambulatory blood pressure values. Darusentan, however, was associated with a high incidence of peripheral edema and fluid retention, a side effect that may reduce the safety profile of the drug and its tolerability. Although these data are promising, the drug requires further evaluation, with particularly regard to the long term [47]. Atrasentan is also a highly selective ERA was found to be beneficial in BP reduction for 72 patients with multiple CV risk factors and non-obstructive coronary artery disease on coronary angiogram [48]. It also had a positive influence on the patients’ metabolic profile.
Novel BP-lowering drugs (nitric oxide donors, vasopressin antagonists, neutral endopeptidase inhibitors, aldosterone synthase inhibitors, etc.) are all undergoing early stages of investigation [49]. It is obvious that further investigations needed with these novel drug categories.
Interventional management of Resistant Hypertension
A significant number of hypertensive subjects fail to achieve adequate BP control despite adherence to maximal doses of several antihypertensive drugs. This situation calls for testing alternative approaches in patients with RH [50-53].
Renal sympathetic nerve ablation is achieved percutaneously via the lumen of the renal artery, using a catheter connected to a radiofrequency generator. It is a minimally invasive, endovascular catheter based procedure. Nerves in the wall of the renal artery are ablated by applying radiofrequency pulses or ultrasound to the renal arteries. This results in reduction of sympathetic afferent and efferent nerve activity to the kidney, so BP can be reduced [53]. The Symplicty HTN 2 trial examined catheter based renal denervation effect on lowering blood pressure in patients with treatment-resistant hypertension. The trial showed effective blood pressure lowering with sympathetic renal denervation [54]. But further study, Symplicity HTN-3, in which 535 patients with severe RH were randomized to undergo renal denervation or a sham procedure (in a 2:1 ratio) did not prove the same findings. The results of the study showed no statistically significant difference between two procedures [55]. After following recent trials it became clear that methodological issues and poor performance and execution of the intervention have hampered the results of Symplicity HTN-3 study, thereby extremely limiting its validity.Following the publication of Symplicity HTN-3 the Joint UK Societies produced a consensus statement that did not recommend the use of renal denervation for treatment of RH in routine clinical practice.
Pekarskiy et al. compared conventional main renal artery denervation with distal renal artery denervation in 51 treatment-resistant hypertensive patients in a single-center, double-blind, randomized, controlled, and parallel group study. Six months after randomization, the distal therapy group (n = 24) had a significantly greater decrease in the primary outcome, 24-h mean ambulatory SBP, as compared with the conventionally treated group (n = 21): -22.6 ± 20.0 vs -9.4 ± 18.7 mmHg; P less than 0.05. No major safety issues were observed in either group [56].
At present, the renal denervation method needs additional data from properly designed long-term comparison trials to conclusively establish its safety and persistent efficacy over the best possible drug treatments. Understanding what makes renal denervation effective or ineffective (patient characteristics or failure to achieve renal sympathectomy) will also be important to avoid the procedure in individuals unlikely to respond [55, 57, 58].
New randomized prospective clinical trials have or will be started soon [59] so that the role of renal denervation will be more clear.
Electrical stimulation of the carotid sinus is also a new interesting approach for the treatment of RH. Arterial baroreceptors are mechanosensitive areas in the walls of the carotid sinuses and aortic arch that buffer the increases and decreases in arterial BP [60]. Baroreceptor stimulation (BAROSTIM) is a technique aimed to decrease BP in RH. BAROSTIM interferes with baroreflex loop by stimulating baroreceptors and afferences of the baroreflex. There is only one randomized controlled trial with this technique which showed a modest but apparently durable BP reduction. Although only a few remediable side-effects of a local nature (infection, nerve damage, pain of glossopharyngeal nerve origin, etc.) have so far been reported, a larger database is also needed to conclusively establish its safety. Ongoing technical improvements to reduce the inconvenience represented by the surgical implantation of the stimulating devices, and to prolong the duration of the battery providing the stimulation, are being tested. More evidences are required to refine the place of BAROSTIM, particularly with new devices [61].
Both the renal denervation and carotid baroreceptor stimulation belongs to a new family of interventional techniques which should be restricted to RH patients at particularly high risk, after fully documenting the inefficacy [1, 61].
The latest non-pharmacological scientific development is lowering BP by creating an arteriovenous anastomosis between the common iliac vein and artery by means of a metal coupler device. The randomized, non-blinded ROX CONTROL HTN study showed that office SBP was reduced by 27 mmHg in patients assigned to arteriovenous coupler therapy, compared with a reduction of 4 mmHg in patients assigned to normal care. As this was not a double-blind, sham-controlled study, caution is needed. Complications related to the procedure or device were seen in 60% of patients in the intervention group. Venous stenosis was the most common complication. There are also concerns about adverse effects. This approach might be a useful adjunctive therapy for patients with uncontrolled hypertension. Questions remain regarding the exact working mechanism, size and duration of the effects on BP [62-64]. Further studies are needed to assess the effects of the procedure.
Follow-up in Resistant Hypertension
RH patients should be monitored closely. Office BP should be measured at frequent intervals and ambulatory BP at least once a year. Organ structure and function measures (especially kidney) also should be examined yearly in order to diagnose probable organ damage at early phase. If the patient uses mineralocorticoid receptor antagonists particularly in a combination with RAS blockers, frequent assessment of serum potassium and creatinine concentration should be done [1].
Conclusion
RH remains a challenging clinical problem with adverse impact on CV events and death, which will increasingly become more common. Effective management of RH requires first, a careful examination and exclusion of factors associated with pseudoresistance, and second, identification and, when possible, modification of factors related to true BP elevations. After all these steps are successfully managed, an aggressive treatment regimen designed to compensate for all mechanisms of BP elevation, most importantly to control volume overload with proper use of diuretics, will help in moving toward effective BP control for the majority of patients. Novel interventional therapies may become a viable option for those patients with uncontrolled hypertension despite receiving an optimal multiple medication, nevertheless additional data for properly designed long term trials is needed.
Şəkillər
Açar sözlər
İstinadlar
1. Mancia, G., et al., 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood pressure, 2013. 22(4): p. 193-278.
2. Boswell, L., J. Pascual, and A. Oliveras, Resistant hypertension: do all definitions describe the same patients&quest. Journal of human hypertension, 2015. 29(9): p. 530-534.
3. Wienemann, H., et al., Treating resistant hypertension with new devices. Minerva Cardioangiol, 2014. 62(3): p. 235-241.
4. Fagard, R.H., Resistant hypertension. Heart, 2012. 98(3): p. 254-261.
5. de la Sierra, A., et al., Clinical features of 8295 patients with resistant hypertension classified on the basis of ambulatory blood pressure monitoring. Hypertension, 2011. 57(5): p. 898-902.
6. Daugherty, S.L., et al., Incidence and prognosis of resistant hypertension in hypertensive patients. Circulation, 2012. 125(13): p. 1635-1642.
7. Persell, S.D., Prevalence of resistant hypertension in the United States, 2003–2008. Hypertension, 2011. 57(6): p. 1076-1080.
8. Judd, E. and D. Calhoun, Apparent and true resistant hypertension: definition, prevalence and outcomes. Journal of human hypertension, 2014. 28(8): p. 463.
9. Tanner, R.M., et al., Prevalence of apparent treatment-resistant hypertension among individuals with CKD. Clinical Journal of the American Society of Nephrology, 2013. 8(9): p. 1583-1590.
10. Calhoun, D.A., et al., Resistant hypertension: diagnosis, evaluation, and treatment a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension, 2008. 51(6): p. 1403-1419.
11. Mancia, G., et al., 2007 ESH-ESC practice guidelines for the management of arterial hypertension: ESH-ESC task force on the management of arterial hypertension. Journal of hypertension, 2007. 25(9): p. 1751-1762.
12. Redon, J., et al., Prognostic value of ambulatory blood pressure monitoring in refractory hypertension A Prospective Study. Hypertension, 1998. 31(2): p. 712-718.
13. Pierdomenico, S.D., et al., Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. American journal of hypertension, 2005. 18(11): p. 1422-1428.
14. Salles, G.F., C.R. Cardoso, and E.S. Muxfeldt, Prognostic influence of office and ambulatory blood pressures in resistant hypertension. Archives of Internal Medicine, 2008. 168(21): p. 2340-2346.
15. Muxfeldt, E.S., C.R.L. Cardoso, and G.F. Salles, Prognostic value of nocturnal blood pressure reduction in resistant hypertension. Archives of Internal Medicine, 2009. 169(9): p. 874-880.
16. Makris, A., M. Seferou, and D.P. Papadopoulos, Resistant hypertension workup and approach to treatment. International journal of hypertension, 2010. 2011.
17. Sarafidis, P.A. and G.L. Bakris, Resistant hypertension: an overview of evaluation and treatment. Journal of the American College of Cardiology, 2008. 52(22): p. 1749-1757.
18. Pickering, T.G., et al., Recommendations for blood pressure measurement in humans and experimental animals part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension, 2005. 45(1): p. 142-161.
19. Erdine, S. and E. Arslan, Monitoring treatment adherence in hypertension. Current hypertension reports, 2013. 15(4): p. 269-272.
20. Moser, M. and J.F. Setaro, Resistant or difficult-to-control hypertension. New England Journal of Medicine, 2006. 355(4): p. 385-392.
21. Redon, J., F. Martinez, and G. Pichtler, RESISTANT AND MALIGNANT HYPERTENSION. Manual of Hypertension of the European Society of Hypertension, 2014: p. 357.
22. Grossman, E. and F.H. Messerli, Secondary hypertension: interfering substances. The Journal of Clinical Hypertension, 2008. 10(7): p. 556-566.
23. Johnson, A., T. Nguyen, and R. Day, Do nonsteroidal anti-inflammatory drugs affect blood pressure? A meta analysis. Journal of Emergency Medicine, 1995. 13(3): p. 430-430.
24. Whelton, A., et al., Effects of celecoxib and rofecoxib on blood pressure and edema in patients≥ 65 years of age with systemic hypertension and osteoarthritis. The American journal of cardiology, 2002. 90(9): p. 959-963.
25. Yakovlevitch, M. and H.R. Black, Resistant hypertension in a tertiary care clinic. Archives of Internal Medicine, 1991. 151(9): p. 1786-1792.
26. Garg, J.P., et al., Resistant hypertension revisited: a comparison of two university-based cohorts. American journal of hypertension, 2005. 18(5): p. 619-626.
27. Sarafidis, P.A. and G.L. Bakris, State of hypertension management in the United States: confluence of risk factors and the prevalence of resistant hypertension. The Journal of Clinical Hypertension, 2008. 10(2): p. 130-139.
28. Gaddam, K.K., et al., Characterization of resistant hypertension: association between resistant hypertension, aldosterone, and persistent intravascular volume expansion. Archives of Internal Medicine, 2008. 168(11): p. 1159-1164.
29. Nishizaka, M.K., M.A. Zaman, and D.A. Calhoun, Efficacy of low-dose spironolactone in subjects with resistant hypertension. American Journal of Hypertension, 2003. 16(11): p. 925-930.
30. De Souza, F., et al., Efficacy of spironolactone therapy in patients with true resistant hypertension. Hypertension, 2010. 55(1): p. 147-152.
31. Chapman, N., et al., Effect of spironolactone on blood pressure in subjects with resistant hypertension. Hypertension, 2007. 49(4): p. 839-845.
32. Engbaek, M., et al., The effect of low-dose spironolactone on resistant hypertension. Journal of the American Society of Hypertension, 2010. 4(6): p. 290-294.
33. Lane, D.A., S. Shah, and D.G. Beevers, Low-dose spironolactone in the management of resistant hypertension: a surveillance study. Journal of hypertension, 2007. 25(4): p. 891-894.
34. Williams, B., et al., Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. The Lancet, 2015. 386(10008): p. 2059-2068.
35. Verdalles, U., et al., Management of resistant hypertension: Aldosterone antagonists or intensification of diuretic therapy? Nephrology, 2015. 20(8): p. 567-571.
36. Oliveras, A., et al., Spironolactone versus sympathetic renal denervation to treat true resistant hypertension: results from the DENERVHTA study–a randomized controlled trial. Journal of Hypertension, 2016. 34(9): p. 1863.
37. Václavík, J., et al., Addition of Spironolactone in Patients with Resistant Arterial Hypertension (ASPIRANT) a randomized, double-blind, placebo-controlled trial. Hypertension, 2011. 57(6): p. 1069-1075.
38. Bobrie, G., et al., Sequential nephron blockade versus sequential renin–angiotensin system blockade in resistant hypertension: a prospective, randomized, open blinded endpoint study. Journal of hypertension, 2012. 30(8): p. 1656-1664.
39. Alvarez-Alvarez, B., et al., Management of resistant arterial hypertension: role of spironolactone versus double blockade of the renin–angiotensin–aldosterone system. Journal of hypertension, 2010. 28(11): p. 2329-2335.
40. Rodilla, E., et al., Spironolactone and doxazosin treatment in patients with resistant hypertension. Revista Española de Cardiología (English Edition), 2009. 62(2): p. 158-166.
41. Oxlund, C.S., et al., Low dose spironolactone reduces blood pressure in patients with resistant hypertension and type 2 diabetes mellitus: a double blind randomized clinical trial. Journal of hypertension, 2013. 31(10): p. 2094-2102.
42. Kota, S.K., et al., Spironolactone treatment in patients with diabetic microalbuminuria and resistant hypertension. International Journal of Diabetes in Developing Countries, 2012. 32(1): p. 33-36.
43. Hermida, R.C., et al., Chronotherapy improves blood pressure control and reverts the nondipper pattern in patients with resistant hypertension. Hypertension, 2008. 51(1): p. 69-76.
44. Minutolo, R., et al., Changing the timing of antihypertensive therapy to reduce nocturnal blood pressure in CKD: an 8-week uncontrolled trial. American Journal of Kidney Diseases, 2007. 50(6): p. 908-917.
45. Tsioufis, C., et al., Managing hypertension in obstructive sleep apnea: the interplay of continuous positive airway pressure, medication and chronotherapy. Journal of hypertension, 2010. 28(5): p. 875-882.
46. Weber, M.A., et al., A selective endothelin-receptor antagonist to reduce blood pressure in patients with treatment-resistant hypertension: a randomised, double-blind, placebo-controlled trial. The Lancet, 2009. 374(9699): p. 1423-1431.
47. Grassi, G., Selective endothelin receptor blockade in resistant hypertension: results of the DORADO trial. Expert opinion on pharmacotherapy, 2011. 12(1): p. 153-155.
48. Raichlin, E., et al., Efficacy and safety of atrasentan in patients with cardiovascular risk and early atherosclerosis. Hypertension, 2008. 52(3): p. 522-528.
49. Laurent, S., M. Schlaich, and M. Esler, New drugs, procedures, and devices for hypertension. The Lancet, 2012. 380(9841): p. 591-600.
50. Doumas, M., D. Guo, and V. Papademetriou, Carotid baroreceptor stimulation as a therapeutic target in hypertension and other cardiovascular conditions. Expert opinion on therapeutic targets, 2009. 13(4): p. 413-425.
51. Doumas, M., C. Faselis, and V. Papademetriou, Renal sympathetic denervation and systemic hypertension. The American journal of cardiology, 2010. 105(4): p. 570-576.
52. Scheffers, I.J., et al., Novel baroreflex activation therapy in resistant hypertension: results of a European multi-center feasibility study. Journal of the American College of Cardiology, 2010. 56(15): p. 1254-1258.
53. Krum, H., et al., Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. The Lancet, 2009. 373(9671): p. 1275-1281.
54. Esler, M.D., et al., Renal sympathetic denervation for treatment of drug-resistant hypertension one-year results from the Symplicity HTN-2 randomized, controlled trial. Circulation, 2012. 126(25): p. 2976-2982.
55. Bhatt, D.L., et al., A controlled trial of renal denervation for resistant hypertension. New England Journal of Medicine, 2014. 370(15): p. 1393-1401.
56. Pekarskiy, S.E., et al., Denervation of the distal renal arterial branches vs. conventional main renal artery treatment: a randomized controlled trial for treatment of resistant hypertension. Journal of Hypertension, 2017. 35(2): p. 369-375.
57. Lobo, M.D., et al., Central arteriovenous anastomosis for the treatment of patients with uncontrolled hypertension (the ROX CONTROL HTN study): a randomised controlled trial. The Lancet, 2015. 385(9978): p. 1634-1641.
58. Schmieder, R.E., et al., ESH position paper: renal denervation–an interventional therapy of resistant hypertension. Journal of hypertension, 2012. 30(5): p. 837-841.
59. Ott, C. and R.E. Schmieder, Renal denervation for resistant hypertension: past, present, and future. Current hypertension reports, 2015. 17(8): p. 1-9.
60. Victor, R.G., Carotid baroreflex activation therapy for resistant hypertension. Nature Reviews Cardiology, 2015. 12(8): p. 451-463.
61. Lantelme, P., B. Harbaoui, and P.-Y. Courand, [Resistant hypertension and carotid baroreceptors stimulation]. Presse medicale (Paris, France: 1983), 2014. 44(7-8): p. 730-736.
62. Lobo, M.D., et al., Joint UK societies’ 2014 consensus statement on renal denervation for resistant hypertension. Heart, 2014: p. heartjnl-2014-307029.
63. Spiering, W. and P. de Leeuw, [Central arteriovenous anastomosis: the solution for patients with treatment-resistant hypertension?]. Nederlands tijdschrift voor geneeskunde, 2014. 159: p. A9129-A9129.
64. Frank, H., et al., Temporary reduction of blood pressure and sympathetic nerve activity in hypertensive patients after microvascular decompression. Stroke, 2009. 40(1): p. 47-51.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 31.Dec.2017
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 1124