

Abstrakt
Sinus pauza Sinus düyününün disfunksiyasının bir forması kimi terapevt və kardioloqların ambulator müayinə zamanı rast gəldiyi qeyri – adi problemlərdən biridir. Əksər hallarda belə xəstələrin heç bir şikayəti olmur. Sinus pauzanın başgicəllənmə, huşun itirilməsi və ya bayılma ilə müşahidə olunması həyat üçün ciddi təhlükə hesab olunur. Bəzi hallarda Sinus pauzamüxtəlif dərmanların mütəmadi və ya nəzarətsiz qəbulu zamanı da müşahidə olunur. Bu klinik müşahidədə, koronar arteriya xəstəliyiolan pasiyentdə Eqilok mualicəsi nəticəsində yaranmış asimptomatik Sinus pauzanın diaqnostikası müzakirə olunacaq.
Əsas mətn
A 41 - year-old male presented with general fatigue for 5 days. There was no associated chest pain, palpitations or syncope. His past history: 7 years ago, when he was practically a healthy person, he was playing football during which he suddenly developed severe typical chest pain and was admitted to CCU. ECG showed acute MI pattern. However, CAG revealed normal coronary anatomy. He was successfully treated as MI patient and after discharging from the hospital was recommended standard routine therapy such as Egilok 50 mg/daily, Escalon 40 mg/daily and Aspirin 100 mg/daily. For the following seven years of his life he had active life style. His weight was 91 kg. He had no hypertension, diabetes and hereditary predisposition. He did not consume alcohol. He was smoker 20 cigarettes a day for about 20 years. The patient continuously for 7 years was treated for the above drugs without medical supervision.
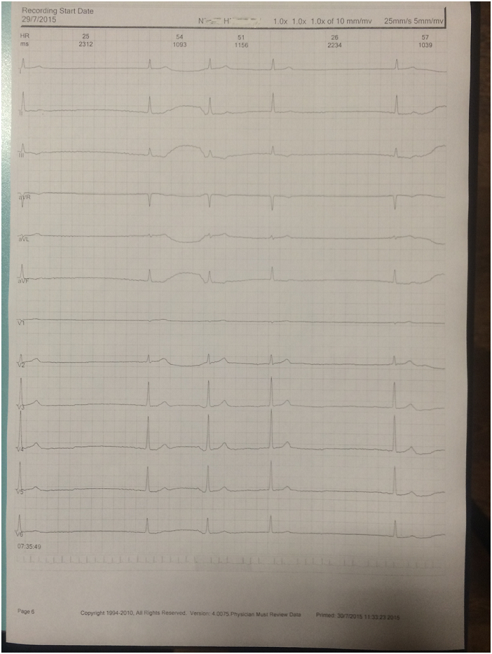
Physical examination did not reveal any significant abnormalities. Two-dimensional echocardiography revealed normal right and left ventricular size and function. Chest X-ray, Blood exam and Thyroid function, also were normal. ECG showed sinus bradycardiya with heart rate 56 BPM. Holter monitoring showed 15 episodes of pauses more than 2.1 sec. and 2 episodes of pauses more than 2.3 sec. We did not think it was preferable to continue the medical treatment with Egilok and we therefore stopped it.
Go to:
Wide complex tachycardias are a commonly encountered entity in coronary care units, intensive care units and emergency departments. Though, these arrhythmias are potentially fatal, they need to recognized first and treated appropriately. Associated physical signs are helpful in this. We present a case of a 54-year-old-female who recently underwent placement of an implantable cardioverter-defibrillator for cardiomyopathy and developed tachycardia.
Discussion
The disorders that characterize SND include: sinus bradycardia - the heart beats very slowly, less than 60 beats per minute; sinus arrest or sinus pause is defined as absence of sinus P waves on the ECG for more than 2 seconds due to a lack of sinus nodal pacemaker activity. A sinus pause of 2 seconds is not unusual in a healthy person. However, a sinus pause of more than 3 seconds is very uncommon except under certain conditions, such as sleep apnea, hypervagotonia state, or seizure activity; sinoatrial block - the sinus node impulse is blocked fromreaching the atria, the two upper chambers of the heart and tachycardia-bradycardia (or tachy-brady) syndrome. In tachy-brady syndrome, the heart sometimes beats too quickly (tachy) and sometimes beats too slowly (brady). Types of tachycardias include atrial fibrillation, atrial flutter and supraventricular tachycardia. (1, 2)
The clinical manifestations of SND are varied and in some cases are seen not only in cardiac patients and also may be found in practically healthy individuals, sportsmen or in patients, receving b/blockers or other therapy. Given this, the diagnosis of SND can be difficult in asymptomatic patients, without HM. (3,4,5). Among the patients with non-specific symptoms, Holter monitoring has got a significant role, in the primary diagnosis of SND in all patients receving b/bloker therapy for long time.
The ACC and the AHA recommend the Holter analysis for the patients with unexplained syncope, near syncope, palpitations and dizziness, as class I indications, for a symptomatic evaluation. Holter monitoring, usually, is indicated if the aetiology of the SND cannot be determined from the patient's history, physical examination, and resting ECG, but the yield of this instrument is low in the patients whose symptoms occur infrequently (3).
Many author believed , that without medical supervision uncontrolled and long period of therapy with b / blockers may lead to a critical reduction in the heart rate going as low as 30 beats per minute which in turn can lead to sudden cardiac arrest. In our study we observed, one of the forms of SND - sinus poses, induced by b\bloker - egilok theraphy for a long time period. For every physician, it is important to monitor every patient with b/blockers therapy 1 - 2 times a year in cases if the patient does not have any complaints (syncope, palpitations or other pure symptoms). This case showed, that HM is an important diagnostic procedure must be used in all patients, which have been treated with b/blockers drugs for a long time.
Conclusion:
B / blockers are one of the most effective drugs for the treatment of coronary artery disease. Its use may be limited by the appearance of a variety of side effects, such as various forms of sinus node dysfunction. SND in some cases may be not found in patents receving b/blokers therapy during resting - short time ECG recording. In these patients life threatening types of SND may be detected only during long time ECG recording. The patients with SND have potential risk for sudden cardiac death and it is important long time ECG (Holter) monitoring for every patient receving b/blokers therapy.
Şəkillər
Açar sözlər
İstinadlar
1. ACC/AHA. Guidelines For Ambulatory Electrocardiography. JACC. 1999;34(3):912–48.
2. Olgin JE, Zipes DP. Specific arrhythmias: Diagnosis and treatment. In RO Bonow et al., eds., Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 9th ed., vol. 1, pp. 771-824. 2012 Philadelphia: Saunders.
3. Zimetbaum PJ, Josephson ME. The Evolving Role of Ambulatory Arrhythmia Monitoring in General Clinical Practice. Annals of Internal Medicine. 1999;130:848–56.
4. Gavin Y Oudit at al. Lithium-induced sinus node disease at therapeutic concentrations: Linking lithium-induced blockade of sodium channels to impaired pacemaker activity. Can J Cardiol. 2007 Mar 1; 23(3): 229–232.2.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 30.Dec.2015
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 1406