

Abstrakt
Ventrikular ekstrasistolalar təcili yardım, koronar və intensiv terapiya bloklarında ən çox rast gəlinən hallardan biridir. Bu aritmiyaların bəzi formaları həyat üçün təhlükəli hesab olunur, dərhal diaqnostika və müvafiq müalicə tələb edir. Çox təəssüf ki, nəinki xəstələrdə, hətta bəzən praktiki sağlam insanlarda da bu aritmiyalar aşkar edilir. Bəzən belə pasiyentlərin anamnezində həyat üçün təhlükəli Ventrikulyar ekstrasistolalar olmur, ya əlamətsiz olur, ya da ki, atipik əlamətlərlə müşahidə edilir. Diqqətinizə çatdırmaq istədiyim 39 yaşlı praktiki sağlam pasiyentdə də fasiləsiz EKQ monitorinq zamanı gün ərzində dəfələrlə həyat üçün təhlükəli olan i ventrikular aritmiya epizodları, əsasən gısa müddətli ventricular taxikardiyalar qeyd olunmuşdur. Bu klinik müşahidədə, asimptomatik ventrikulyar taxikardiyala epizodlarının qeyd olunmasında Holter monitorinqin diaqnostik əhəmiyyəti müzakirə olunacaq.
Əsas mətn
A 39-year-old male presented with continuous pain on the left subscapular area for one month. There was no associated chest pain, palpitations or syncope. Her past history was not for arrhythmias or other heart disorder. His life style is active, weight – 71 kg, he had not hypertension, diabetes and hereditary predisposition. He used alcohol non regular and was not smoker. Physical examination did not suggest any significant abnormalities. Two-dimensional echocardiography revealed normal right and left ventricular size and function. Chest X-ray, Blood exam and Thyroid function, also were normal. Only ventricular premature complexes were observed on the ECG. Holter monitoring showed more than 14945 PVC per 23 hours, especially 1020 V – Runs and 2103 V- Couplet with V-Triplet episodes. Coronary angiography revealed normal coronary anatomy. We do not prefered medical treatment. Patient successfully treated with catheter ablation and PVC was disappeared.
Go to:
Wide complex tachycardias are a commonly encountered entity in coronary care units, intensive care units and emergency departments. Though, these arrhythmias are potentially fatal, they need to recognized first and treated appropriately. Associated physical signs are helpful in this. We present a case of a 54-year-old-female who recently underwent placement of an implantable cardioverter-defibrillator for cardiomyopathy and developed tachycardia.
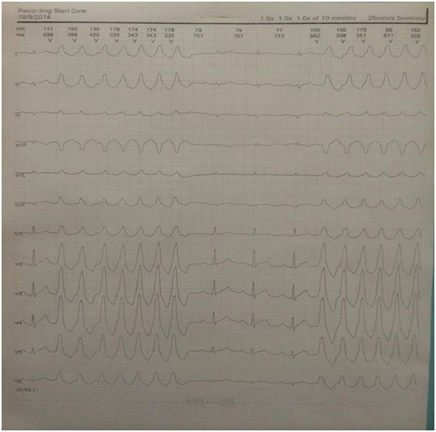
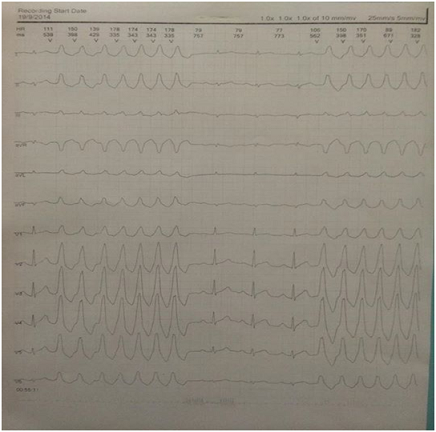
Fig. 1.V – runs episode, before night sleeping at 00.55.11
Fig. 2. V- couplet and V - triplet episodes, 05.01.02 at night sleeping time
Fig. 3.V – runs episode, morning time at 08.45.11.
Discussion
Arrhythmias can be life-threatening if they cause a severe decrease in the pumping function of the heart. When the pumping function is severely decreased for more than a few seconds, blood circulation is essentially stopped, and organ damage may occur within a few minutes. Arrhythmias are identified by where they occur in the heart (atria or ventricles) and by what happens to the heart's rhythm when they occur. Arrhythmias that start in the atria are called atrial or supraventricular (above the ventricles) arrhythmias. Ventricular arrhythmias begin in the ventricles. Ventricular arrhythmias are usually caused by heart disease are very serious. PVCs are characterized by premature and bizarrely shaped QRS complexes usually wider than 120 msec. with the width of the ECG. These complexes are not preceded by a P wave, and the T wave is usually large, and its direction is opposite the major deflection of the QRS. PVCs are common with an estimated prevalence of 1% to 4% in the general population. In a normal healthy population, PVCs have been detected in 1% of subjects on standard 12-lead electrocardiography and between 40% and 75% of subjects on 24- to 48-hour Holter monitoring.
Life-threatening PVC include ventricular tachycardia and ventricular fibrillation.
One of the type of V – tach is V – Runs or Nonsustained ventricular tachycardia (NSVT). V – Runs is defined as 3 (sometimes 5) or more consecutive beats arising below the atrioventricular node with an RR interval of <600 ms (>100 beats/min) and lasting <30 s (1). This definition, however, is not universal. V – Runs has also been defined as runs of ≥16 beats with a rate ≥125 beats/min (2) or >120 beats/min (3), using a time cutoff of 15 s (4), or even without strictly defined diagnostic criteria (5). Thus, reliable epidemiological data on V – Runs are difficult to obtain, particularly because reproducibility of V – Runs recordings on HM is documented in only half of the patients with this arrhythmia (6). Although V – Runs may cause symptoms of palpitations, usually it is asymptomatic because of its brevity and the nature of the short-lived episodes of arrhythmia may not allow a clear distinction between monomorphic and polymorphic ventricular rhythms. When V – Runs is documented in the context of a history of established monomorphic V - Tach, it is usually monomorphic and may demonstrate the same morphology and share the same mechanism with the clinical sustained arrhythmia, especially in cases of idiopathic V - Tach.
In several clinical settings, V – Runs is a marker of increased risk for subsequent sustained tachyarrhythmias and SCD, whereas it may have no prognostic significance in others. The important tasks of the physician are to detect those apparently healthy individuals in whom NSVT represents a sign of occult disease, and to risk-stratify patients with known disease who present with this arrhythmia to provide therapy that mitigates associated risks. This may not always be easy in clinical practice. Whether NSVT provokes sustained, life-threatening arrhythmias or is simply a surrogate marker of a more severe underlying pathology is still unknown in most clinical settings.
In several clinical settings, NSVT is a marker of increased risk for subsequent sustained tachyarrhythmias and SCD, whereas it may have no prognostic significance in others. The important tasks of the physician are to detect those apparently healthy individuals in whom NSVT represents a sign of occult disease, and to risk-stratify patients with known disease who present with this arrhythmia to provide therapy that mitigates associated risks. This may not always be easy in clinical practice. Whether NSVT provokes sustained, life-threatening arrhythmias or is simply a surrogate marker of a more severe underlying pathology is still unknown in most clinical settings.
In asymptomatic, apparently healthy persons, NSVT episodes may be recorded at rest (7,8,9). Although Framingham data have suggested an association with increased mortality (7), especially in persons with left ventricular hypertrophy (8), the prognostic significance of spontaneous V – Runs recorded in apparently healthy individuals has not been established (9). Recent data have demonstrated that runs of ≥2 consecutive ventricular depolarizations during exercise or at recovery may occur in up to 3% of healthy men and predict an increase in cardiovascular mortality within the next 23 years by a factor of more than 2.5 (10). Frequent ventricular ectopy during recovery after exercise is a better predictor of an increased risk of death than ventricular ectopy occurring only during exercise (11).
V – Runsepisodes may also be recorded in professional athletes without structural heart disease but is considered benign and without long-term implications when suppressed by exercise (12,13,14). Arrhythmia episodes decrease during periods of deconditioning, and resumption of training is safe (15,16). The mechanism of V – Runs in this setting is unknown. A shift of autonomic modulation from parasympathetic to sympathetic predominance induced by intensive endurance training and sinus bradycardia–induced ventricular ectopy have been postulated (15). V – Runs in athletes is considered part of the “athlete's heart syndrome” (12,15) and has no adverse prognostic significance, provided conditions such as hypertrophic cardiomyopathy, early repolarization syndrome, and other genetic channelopathies are excluded. The early repolarization pattern, manifested as QRS slurring or notching, has long been considered to be a benign ECG manifestation that is seen more commonly in young healthy men and athletes (17), but there has been evidence suggesting that it may be associated with a risk for ventricular fibrillation (VF), depending on the magnitude of the J wave and degree of ST ele -vation (18,19,20,21,22). A horizontal/descending type (defined as ≥0.1 mV elevation of the ST segment within 100 ms after the J point) may help to identify those individuals who are clearly at risk (23). V – Runshas been recorded in a wide range of conditions, from apparently healthy individuals to patients with significant heart disease. In the absence of heart disease, the prognostic significance of V – Runs is debatable. When detected during exercise, and especially at recovery, V – Runs indicates increased cardiovascular mortality within the next decades. In trained athletes, V – Runs is considered benign when suppressed by exercise. In patients with non–ST-segment elevation acute coronary syndrome, V – Runs occurring beyond 48 h after admission indicates an increased risk of cardiac and sudden death, especially when associated with myocardial ischemia. In acute myocardial infarction, in-hospital V – Runs has an adverse prognostic significance when detected beyond the first 13 to 24 h. In patients with prior myocardial infarction treated with reperfusion and beta-blockers, V – Runs is not an independent predictor of long-term mortality when other covariates such as left ventricular ejection fraction are taken into account. In patients with hypertrophic cardiomyopathy, and most probably genetic channelopathies, V – Runs carries prognostic significance, whereas its independent prognostic ability in ischemic heart failure and dilated cardiomyopathy has not been established. The management of patients with V – Runs is aimed at treating the underlying heart disease.
Conclusion:
This case described here illustrate the pure variety in clinical presentation of PVC. The clinical manifestations of PVC are varied and is seen not only in cardiac patients and also found in practically healthy individuals and sportsmen. Therefore, the diagnosis different forms of life-threatening PVC can be difficult in such category patients, without HM. For every physician, it is important to be aware of this arrhythmias when a patient is not presents with syncope, palpitations or other pure symptoms. This case showed, that HM as a important diagnostic procedure, must be used as routine not only in cardiac patients, and also in asymptomatic individuals, sportsmen and practically healthy persons.
Acknowledgments:
The author would like to thank Rauf Khalilov for the editoral support
Şəkillər
Açar sözlər
İstinadlar
1. Katritsis D.G., Camm A.J.; Nonsustained ventricular tachycardia: where do we stand? Eur Heart J. 2004;25:1093-1099.
2. Bloch Thomsen P.E., Jons C., Raatikainen M.J., Long-term recording of cardiac arrhythmias with an implantable cardiac monitor in patients with reduced ejection fraction after acute myocardial infarction: the Cardiac Arrhythmias and Risk Stratification After Acute Myocardial Infarction (CARISMA) study. Circulation. 2010;122:1258-1264.
3. Grimm W., Christ M., Bach J., Müller H.H., Maisch B.; Noninvasive arrhythmia risk stratification in idiopathic dilated cardiomyopathy: results of the Marburg cardiomyopathy study. Circulation. 2003;108:2883-2891.
4. Caruso A.C., Marcus F.I., Hahn E.A., Hartz V.L., Mason J.W.; Predictors of arrhythmic death and cardiac arrest in the ESVEM trial. Circulation. 1997;96:1888-1892.
5. Teerlink J.R., Jalaluddin M., Anderson S., Ambulatory ventricular arrhythmias in patients with heart failure do not specifically predict an increased risk of sudden death. Circulation. 2000;101:40-46.
6. Senges J.C., Becker R., Schreiner K.D., Variability of Holter electrocardiographic findings in patients fulfilling the noninvasive MADIT criteria. Pacing Clin Electrophysiol. 2002;25:183-190.
7. Bikkina M., Larson M.G., Levy D.; Prognostic implications of asymptomatic ventricular arrhythmias: the Framingham heart study. Ann Int Med. 1992;117:990-996.
8. Bikkina M., Larson M.G., Levy D.; Asymptomatic ventricular arrhythmias and mortality risk in subjects with left ventricular hypertrophy. J Am Coll Cardiol. 1993;22:1111-1116.
9. Engstrom G., Hedblad B., Janzon L., Ventricular arrhythmias during 24-h ambulatory ECG recording: incidence, risk factors and prognosis in men with and without a history of cardiovascular disease. J Intern Med. 1999;246:363-372.
10. Jouven X., Zureik M., Desnos M., Courbon D., Ducimetiere P.; Long-term outcome in asymptomatic men with exercise-induced premature ventricular depolarizations. N Engl J Med. 2000;343:826-833.
11. Frolkis J.P., Pothier C.E., Blackstone E.H., Lauer M.S.; Frequent ventricular ectopy after exercise as a predictor of death. N Engl J Med. 2003;348:781-790.
12. Biffi A., Pelliccia A., Verdile L., Long-term clinical significance of frequent and complex ventricular tachyarrhythmias in trained athletes. J Am Coll Cardiol. 2002;40:446-452.
13. Baldesberger S., Bauersfeld U., Candinas R., Sinus node disease and arrhythmias in the long-term follow-up of former professional cyclists. Eur Heart J. 2008;29:71-78.
14. Biffi A., Maron B.J., Di Giacinto B., Relation between training-induced left ventricular hypertrophy and risk for ventricular tachyarrhythmias in elite athletes. Am J Cardiol. 2008;101:1792-1795.
15. Biffi A., Maron B.J., Verdile L., Impact of physical deconditioning on ventricular tachyarrhythmias in trained athletes. J Am Coll Cardiol. 2004;44:1053-1058.
16. Biffi A., Maron B.J., Culasso F., Patterns of ventricular tachyarrhythmias associated with training, deconditioning and retraining in elite athletes without cardiovascular abnormalities. Am J Cardiol. 2011;107:697-703.
17. Surawicz B., Macfarlane P.W.; Inappropriate and confusing electrocardiographic terms J-wave syndromes and early repolarization. J Am Coll Cardiol. 2011;57:1584-1586.
18. Antzelevitch C., Yan G.X.; J wave syndromes. Heart Rhythm. 2010;7:549-558.
19. Tikkanen J.T., Anttonen O., Junttila M.J., Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009;361:2529-2537.
20. Haissaguerre M., Derval N., Sacher F., Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008;358:2016-2023.
21. Watanabe H., Makiyama T., Koyama T., High prevalence of early repolarization in short QT syndrome. Heart Rhythm. 2010;7:647-652.
22. Cappato R., Furlanello F., Giovinazzo V., J wave, QRS slurring, and ST elevation in athletes with cardiac arrest in the absence of heart disease: marker of risk or innocent bystander?. Circ Arrhythm Electrophysiol. 2010;3:305-311.
23. Tikkanen J.T., Junttila M.J., Anttonen O., Early repolarization: electrocardiographic phenotypes associated with favorable long-term outcome. Circulation. 2011;123:2666-2673.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 30.Dec.2015
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 1977