

Abstrakt
Məqsəd: Bu tədqiqatın məqsədi müalicəyə çətin tabe olan xəstələr arasında arterial təzyiqə nəzarət üçün 3 preparatdan ibarət antihipertenziv strategiyanı qiymətləndirmək idi. Dizayn: PIANIST tədqiqatı (The Perindopril-Indapamide plus AmlodipiNe in high risk hyperTensive patients) xəstələr üzərində 4 aylıq müşahidəni nəzərdə tuturdu. Xəstələr: Tədqiqata, aldıqları terapiyaya baxmayaraq tam yaxşı nəzarət olunmayan, yüksək və çox yüksək ürək-damar riski olan, hipertoniyalı, eləcə də aldıqları perindopril 10 mq / indapamid 2.5 mq fiksə kombinasiyası ilə müalicə strategiyası əsasında amlodipin 5 və ya 10 mq əlavə olunması planlaşdırılan xəstələr də daxil olmaqla, ümumilikdə 4 731 xəstə cəlb olunmuşdu.
Əsas mətn
The morbidity and mortality challenges associated with long-term hypertension are such that controlling blood pressure has become a significant focus in global public health [1, 2]. Over the last 10 years, advancements in awareness and treatment strategies and changes in guidelines to include dual therapies have improved blood pressure control rates [3, 4]. However, a significant need to develop safer, more efficacious blood pressure control strategies still exists [5, 6].
As additional reductions in blood pressure and morbi-mortality have been found with triple drug therapies compared with dual therapies and with single-pill formulations compared with free associations [7, 8], guidelines continue to support single-pill formulations and combinations that target multiple pathophysiological pathways and inhibit feedback loops [9]. The perindopril/indapamide/amlodipine combination is one possible triple-drug combination in which the calcium channel blocker (CCB) amlodipine and the diuretic indapamide mediate natriuresis and stimulate renin activity, while the angiotensin-converting enzyme (ACE) inhibitor perindopril inhibits the renin–angiotensin–aldosterone system (RAAS). Based on the current understanding of hypertension, the simultaneous targeting of these pathways would be expected to re-establish the balance between renin and sodium and, as a result, decrease blood pressure control and reduce adverse event rates generated by any one therapeutic class.
The combination of perindopril/indapamide/amlodipine is also supported by extensive blood pressure and clinical outcome data [10–19]. In particular, results from the ASCOT (Anglo-Scandinavian Cardiac Outcomes Trial), HYVET (Hypertension in the Very Elderly), and ADVANCE (Action in Diabetes and Vascular Disease) trials suggest that, in addition to the blood pressure-lowering benefits, a perindopri/indapamide/amlodipine combination is likely to reduce mortality [12, 14, 18, 20, 21].
Consistent with these efficacy and tolerability expectations, data from the observational PIANIST trial, in which 12,064 patients with blood pressure that was not properly controlled were treated with a free combination of perindopril/indapamide/amlodipine, showed that after 4 months of treatment, significant changes from baseline in blood pressure were noted [22]. In the current study, we evaluated the efficacy and tolerability of single-pill perindopril/indapamide in free association with amlodipine in high- to very high-risk patients with essential hypertension that was not properly controlled despite previous treatment. The aim of this study was to evaluate this triple therapy in order to support the development of a safe and efficacious triple-drug fixed combination formulation and in order to offer an ACE inhibitor-containing alternative to currently marketed triple-drug therapy single pill combinations, all of which include an angiotensin receptor blocker (ARB).
1.Metods
2.1 Study Design
In this multicenter, prospective, observational, non-interventional, 4 month, open label clinical study named PIANIST (Perindopril-Indapamide plus AmlodipiNe in high rISkhyperTensive patients), patients at high or very high cardiovascular risk were enrolled if they had essential hypertension that was not properly controlled despite anti-hypertensive therapy. Patients were switched to treatment with fixed-dose combination perindopril 10 mg/indapamide 2.5 mg with the co-administration of amlodipine (2.5, 5.0, or 10 mg). As this was a non-interventional, observational trial, physicians (internists, hypertension specialists, cardiologists, or family practitioners) only enrolled patients for whom the switch to study drug was consistent with their existing therapeutic plan and in line with the summary of (registration numbers: OGYI-T-20300 and OGYI-T-07604). Additional antihypertensive therapies were allowed. A subset of patients were, at the physician’s discretion, enrol- led in the ambulatory blood pressure monitoring (ABPM) substudy. This study was performed in accordance with the ethical standards described in the Declaration of Helsinki (1964; 1975; 1983) and was approved by the appropriate ethics committee (approval number by ETT-TUKEB-NIT: 31599/2011/EKU 936/PI/ll).
2.2 Inclusion/Exclusion Criteria
Ambulatory patients who were over 18 years of age were enrolled if they had essential hypertension that was not properly controlled despite ongoing antihypertensive treatment and were at high or very high cardiovascular risk. Cardiovascular risk was defined as outlined in 2007 hypertension guidelines of the European Society of Cardiology/European Society of Hypertension [11].
In addition, women needed to be using an effective method of contraception or to have been postmenopausal for at least 1 year. All patients needed to have provided written informed consent. Patients were excluded if they had any contraindications to perindopril/indapamide or amlodipine, as set out in the summary of product characteristics (registration numbers: OGYI-T-20300 and OGYI- T-07604).
2.2. Measurements
Patients attended three visits (inclusion/baseline, month 1, and month 4). Patient history was collected during the baseline visit. Blood pressure and heart rate were collected at the physician’s office at baseline, month 1, and month 4. Blood pressure was measured according to the 2009 Hungarian Society of Hypertension management guide- lines [23]. Laboratory parameters (total cholesterol, low-density lipoprotein [LDL] cholesterol, high-density lipoprotein [HDL] cholesterol, triglycerides, fasting glucose, hemoglobin A1c, serum creatinine, uric acid, microalbuminuria, estimated glomerular filtration rate [eGFR], potassium, and sodium) were determined at the discretion of the physician at baseline and month 4. Adverse events were recorded on case report forms at month 1 and month 4.
2.2 Statistics
Data were collected and analyzed according to European Guidelines for Good Clinical Practice/International Conference on Harmonisation (ICH) standards. As the aim of the study was to evaluate the efficacy of the triple drug combination perindopril 10 mg/indapamide 2.5 mg/ amlodipine 5 or 10 mg, only patients taking these dosages of medication and for whom all blood pressure and heart rate data were available were included in the main cohort.
Data were analyzed using descriptive statistical methods. For quantitative variables, means and standard deviations are presented; for qualitative variables, n and percentages were calculated. Between-group comparisons were performed using one-sample t tests and Chi-squared tests. Significance for two-sided tests was set at 5 %.
Calculations were performed in the main cohort and in the subgroup of patients who had undergone ABPM. Data were analyzed according to grade of hypertension and preexisting antihypertensive treatment (ACE inhibitor, ARB, ACE inhibitor+hydrochlorothiazide, ARB+hydrochlorothiazide, amlodipine, ACE inhibitor + amlodipine; ARB + amlodipine). Grade of hypertension was defined according to the 2007 hypertension guidelines of the European Society of Cardiology/European Society of Hypertension [11]: patients had grade 1 hypertension if their systolic blood pressure (SBP) was between 140 and 159 mmHg or their diastolic blood pressure (DBP) was between 90 and 99 mmHg; patients had grade 2 hypertension if their SBP was between 160 and 179 mmHg or their DBP was between 100 and 109 mmHg; patients had grade 3 hypertension if their SBP was C180 mmHg or their DBP was C110 mmHg.
Target office blood pressure was defined as SBP/ DBP 140/90 mmHg. For ABPM, blood pressure control was defined as SBP/DBP <130/80 mmHg for 24-h blood pressure, <135/85 mmHg for daytime blood pressure, and <120/70 mmHg for nighttime blood pressure. Percent time elevation was defined as percentage of time over a 24-h period during which blood pressure was above 140/90 mmHg during the daytime and 120/80 mmHg during the nighttime. Blood pressure load was defined as percentage area under the blood pressure curve above previously defined values.
2. Results
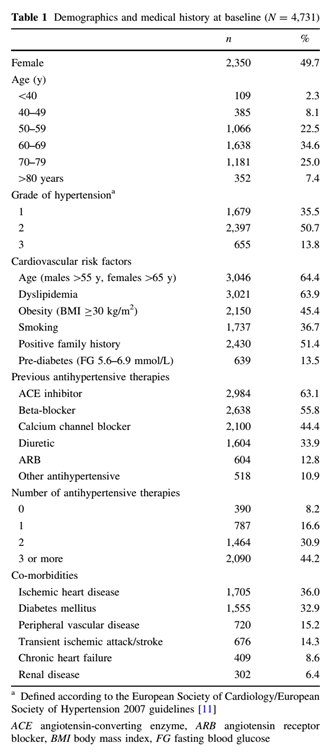
The trial was conducted between 17 February 2012 and 18 September 2012, and was carried out at 762 centers in Hungary. Of the 10,163 patients enrolled in the PIANIST study, 5,432 were excluded from the analysis due to undocumented/other dose of amlodipine (n = 3,675), no evidence of high risk (n = 945), missing data for SBP/ DBP/heart rate (n = 482), missing case report forms/mis- sed visits (n = 181), and patient gender unknown or age unknown/less than 18 years (n = 149). Patients who met study and treatment dose criteria (perindopril 10 mg/ indapamide 2.5 mg/amlodipine 5 or 10 mg) were included in the analysis (N = 4,731). Fifty percent of patients were female (Table 1). Mean age was 63.8 ± 11.1 years and mean body mass index was 29.9 ± 5.3 kg/m2. The proportion of patients with cardiovascular risk factors or target organ damage was high: dyslipidemia (63.9 %), family history of cardiovascular disease (51.4 %), obesity (45.4 %), smoking (36.7 %), ischemic heart disease (36.0 %), diabetes (32.9 %), peripheral artery disease (15.2 %), cerebrovascular disease (14.3 %), pre-diabetes (13.5 %), chronic heart failure (8.6 %), and chronic kidney disease (6.4 %). Patients were being treated with ACE inhibitors (63.1 %), beta-blockers (55.8 %), CCBs (44.4 %), diuretics (33.9 %), ARBs (12.8 %), or other antihypertensive medications (10.9%), and more specifically with amlodipine (39.9%), perindopril (23.3%), hydrochlorothiazide (10.7%), and indapamide (4.5%). Mean baseline office blood pressure was 160.5 ± 13.3 / 93.8 ± 8.7 mmHg and mean duration of hypertension was 11.9 ± 8.2 years. Most patients had grade 2 hypertension (50.7% of patients), followed by grade 1 hypertension (35.5% of patients), and grade 3 hypertension (13.8% of patients). Most patients were receiving two or more antihypertensive medications (75.1%). Mean baseline office heart rate was 79.3 ± 9.2 bpm. In addition to perindopril 10 mg/indapamide 2.5 mg, 19.3 % of patients were prescribed 10 mg of amlodipine at baseline (vs. 80.7 % receiving 5 mg amlodipine); 28.4% of patients were receiving 10 mg of amlodipine at month 1 (vs. 71.6% receiving 5 mg amlodipine); and 29.0% of patients were receiving 10 mg of amlodipine at month 4 (vs. 71.0% receiving 5 mg amlodipine).
3.1 Office Blood Pressure and Heart Rate
After 4 months of therapy, mean office blood pressure had decreased by 28.3 ± 13.5/13.8 ± 9.4 to 132.2 ± 8.6 /80.0 ± 6.6 mmHg (p< 0.0001; Fig.1a), and mean heart rate had decreased by 5.8 ± 8.2 to 73.5 ± 6.2 bpm (p< 0.0001). Significant decreases in blood pressure from baseline occurred regardless of the grade of baseline hyper- tension, with decreases in SBP/DBP of 18.7 ± 8.3 / 9.7 ± 7.2 mmHg for grade 1 patients, 30.4 ± 10.1 / 14.7 ± 8.6 mmHg for grade 2 patients, and 45.4 ± 15.1 / 20.7 ± 12.1 mmHg for grade 3 patients (all p< 0.0001). Significant decreases from baseline in blood pressure also occurred regardless of previous antihypertensive treatment (Fig. 1b)with decreases in blood pressure of 29.3 ± 13.8/13.8 ± 8.5 mmHg in patients previously treated with ACE inhibitors, 29.1 ± 14.5/-15.2 ± 10.9 mmHg in patients previously treated with ARBs, 28.2 ± 13.2/13.6 ± 9.6 mmHg in patients previously treated with ACE inhibitor + hydrochlorothiazide, 25.5 ± 9.8/14.4 ± 9.0 mmHg in patients previously treated with ARB + hydrochlorothiazide, 24.1 ± 10.8/11.6 ± 8.0 mmHg in patients previously treated with amlodipine, 25.4 ± 11.3/11.9 ± 8.2 mmHg in patients previously treated with amlodipine + ACE inhibitor, and 28.2 ± 13.7/14.5 ± 8.5 mmHg in patients previously treated with amlodipine + ARB (for all changes from baseline (p< 0.0001). Significant decreasesdata were analyzed in patients rom baseline in blood pressure occurred regardless of the number of previous antihypertensive treatments, with decreases in blood pressure of 31.7 ± 15.2/15.1 ± 10.2 in previously untreated patients, of 28.1 ± 13.6/13. 6 ± 9.5 in patients previously receiving monotherapy, of 27.6 ± 12.5/13.4 ± 8.9 in patients previously receiving dual therapy, and 28.3 ± 13.8/13.9 ± 9.6 in patients previously treated with three or more antihypertensives (for all changes from baseline p<0.0001). Significant decreases in heart rate were also noted regardless of antihypertensive treatment and number of previous antihypertensive treatments (data not shown)
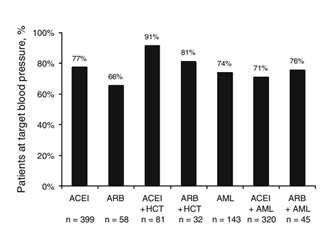
Blood pressure targets were reached by 72.0% of patients in the main cohort, 85.7% of patients with grade 1 hypertension, 69.5% of patients with grade 2 hypertension, and 46.3% of patients with grade 3 hypertension. When according to previous treatments (Fig. 2), 81 and 91% of patients previously treated with an ACE inhibitor/hydrochlorothiazide or an ARB/hydrochlorothiazide reached blood pressure targets, respectively. When blood pressure targets were analyzed according to the number of previous antihypertensive treatments, blood pressure control was reached by 68.2 % of previously untreated patients, 73.8 % of patients previously receiving monotherapy, 73.3 % of patients previously receiving dual therapies, and 71.2 % of patients previously receiving three or more antihypertensive therapies. 73.3% of patients previously receiving dual therapies, and 71.2% of patients previously receiving three or more antihypertensive therapies.
3.2 Ambulatory Blood Pressure Monitoring
In the subgroup of 104 patients who underwent ABPM (Fig. 3), 24-h mean blood pressure decreased over 4 months of treatment from 147.4 ± 13.8/82.1 ± 11.9 to 122.6 ± 9.1/72.8 ± 7.4 mmHg (p\ 0.0001) and heart rate from 73.2 ± 9.9 to 71.1 ± 8.5 bpm (p = 0.03). Twenty-four hour blood pressure targets were reached by 72.1 % of patients. Decreases in daytime and nighttime blood pressure and heart rate were also statistically significant: 79.8 and 51.0 % of patients reached blood pressure targets, respectively. Percent time elevation decreased significantly from 69.5 ± 24.9 to 21.7 ± 18.7 % for SBP (decrease of 47.8 ± 27.6 %; p< 0.0001) and from 42.2 ± 31.3 to 11.9 ± 14.8 % for DBP (decrease of 30.4 ± 29.6 %; p< 0.0001). Changes in blood pressure load were also significant as it decreased from 340.6 ± 289.5 to 56.0 ± 63.0 mmHgh (decrease of 284.6 ± 280.4 mmHgh; p< 0.0001) for SBP and 125.9 ± 168.8 to 19.7 ± 27.3 mmHgh for DBP (decrease of 106.2 ± 159.6 mmHgh; p<0.0001). When data were further analyzed by baseline grade of hypertension, 24-h mean blood pressure decreased by 18.7 ± 10.0/5.0 ± 12.6 mmHg in the grade 1 group from a baseline of 141.2 ± 6.0/77.7 ± 12.7 (n = 19; p = 0.02), by 24.9 ± 12.2/9.2 ± 10.4 mmHg in the grade 2 group from a baseline of 146.4 ± 11.3/81.6 ± 10.5 (n = 64; p<0.0001), and by 30.0 ± 1.5/13.2 ± 11.7 mmHg in the grade 3 group from a baseline of 155.9±20.7/ 87.6 ± 13.8 (n = 21; p = 0.0003). Heart rate decreased by a mean of 3.6 ± 6.9 bpm from a baseline of 74.1 ± 8.6 (p=0.03), 2.7 ± 11.0 bpm from a baseline of 73.5±10.1 (p=0.04), and 1.0±12.9 bpm from a baseline of 71.6 ± 10.6 (p = 0.7) in the grade 1, 2, and 3 groups, respectively. Twenty-four hour blood pressure targets were reached by 79.0, 75.0, and 57.1% of patients in the grade 1, 2, and 3 groups, respectively.
3.3 Laboratory Parameters
Mean changes in sodium and potassium were not clinically significant (Table 2). Improvements in plasma levels oftotal cholesterol (-9.5%), LDL cholesterol (-0.4%), triglycerides (-11.5%), fasting glucose (-4.9%), hemoglobin A1c (-0.3%), serum creatinine (-2.3%), uric acid (-3.5%), microalbuminuria (-28.0%), HDL cholesterol (+3.7%), and eGFR (+1.2%) were noted.
3.4 Safety Thirty-five patients reported a total of 38 adverse events, three of which were serious. The most frequently reported adverse events were ankle edema (n = 9; 0.2% of patients), hypotension (n = 6; 0.1% of patients), cough (n = 4; 0.08%), and dizziness (n = 4; 0.08%). The three serious adverse events that occurred (atrial fibrillation, stroke, and cerebral tumor) were considered unlikely to be related to study treatment.
4. Discussions
In this observational, every day practice, 4-month, openlabel, clinical study of patients at high and very high cardiovascular risk, blood pressure control was significantly improved after 4 months of treatment with triple-drug combination perindopril 10 mg/indapamide 2.5 mg/amlodipine 5 or 10 mg. In these patients with difficult-to-treat hypertension who had been treated unsuccessfully with a wide range of antihypertensives, the switch to perindopril/indapamide/amlodipine led to a mean blood pressuredecrease of 28.3/13.8 mmHg and an overall blood pressurecontrol rate of 72 %. Adverse events, including edema, cough, and headache, were infrequent, and potassium levels were stable. Despite the difficulties associated with treating high-risk patients, significant reductions in blood pressure werenoted 1 month after the switch to perindopril/indapamide/ amlodipine. Since 1-month response rates have been shown to be predictive of long-term cardiovascular events and survival [24], these data suggest that this triple-drug combination may have significant long-term benefits. In addition, significant reductions in blood pressure variability also suggest a likely long-term reduction in morbidity and mortality, as fluctuations in blood pressure over the course of a day have been shown to contribute significantly to end organ damage and cardiovascular risk [25].
Beyond the therapeutic class effects, the specific properties of perindopril, indapamide, and amlodipine suggest additional morbi-mortality benefits [15, 26, 27]. The combination of perindopril with indapamide has been shown to improve vascular endothelial function and target organ function and to decrease the risk of cerebrovascular and cardiovascular events [12, 13, 17–19, 28, 29]. The combination of perindopril with amlodipine has been shown to improve arterial stiffness and wave reflection, as well as cardiovascular outcomes such as stroke and coronary events [14, 30]. Lastly, unlike other ACE inhibitors or ARBs, perindopril plus indapamide sustained release (SR) in the HYVET trial, perindopril in fixed combination with indapamide in the ADVANCE trial, and perindopril in combination with amlodipine in the blood pressure-lowering arm of the ASCOT trial have shown additional and significant mortality benefits [20]. Long-term studies would be needed to confirm that the predicted improvements in organ protection and reduced mortality rates would extend to this triple-drug therapy. The simultane ous targeting of the RAAS and natriuresis pathways was expected to lead to good tolerability. Indeed, the opposing effects of these three drugs are visible in the low adverse event rates. Edema rates (0.2 %) were low, reflecting opposing effects of perindopril and amlodipine on renin [31]; cough rates (0.08 %) were low, reflecting opposing effects of amlodipine on ACE inhibitor-induced coughs [32]; and no changes in potassium were observed, thereby reflecting the opposing effects of indapamide and perindopril [33, 34]. The low cough rate is also likely to be because perindopril has been shown to be associated with low rates of cough [35], and that 63 % of patients had previously been treated with an ACE inhibitor and would not have been susceptible to the cough associated with new treatment with an ACE inhibitor. The low overall adverse event rate in the study is also likely to reflect the well documented low adverse event profile of indapamide. Unlike thiazide diuretics, indapamidehas been shown to be metabolically neutral and to have little effect on potassium levels and on lipid and glucose profiles [33, 34, and 36]. Although guidelines state that ARBs can also be used as the RAAS inhibitor in triple drug combinations [9], metaanalyses suggest that ARBs perform less well than ACE inhibitors with regards to mortality [20, 37]. In a pooled analysis of 20 cardiovascular morbi-mortality trials (n = 158,998), ACE inhibitors were associated with a 10% reduction in all-cause mortality, whereas no significant reduction in mortality was found with ARB treatment [20]. These data thus suggest that, in patients who have no contraindications for ACE inhibitors, triple combinations with ACE inhibitors may represent a better long-term option than ARBs. Supporting this hypothesis, a recent subanalysis of the blood pressure arm of the ADVANCE trial showed that prescription of perindopril/indapamide in patients receiving a CCB at baseline reduced the relative risk of death by 28 % and of major cardiovascular events by 12 % [21].
4.1 Study Limitations
This study was an uncontrolled, open-label study that lasted 4 months. The data presented herein should therefore be interpreted with the knowledge that a placebo effect could not be assessed.
The reductions in blood pressure in patients with grade 3 hypertension resulted in a mean blood pressure <140/90 mmHg. However, the control rate in this group was only 46.3%. This putative discrepancy between these two sets of data reflects the fact that the standard deviations for this group were large and that these patients constitute the hardest to treat group. The improvements in metabolic parameters that were observed in this study need to be interpreted with caution. Our study design does not allow differentiating between a direct effect of treatment on metabolic parameters and a secondary effect, because ewer antihypertensives with unfavorable metabolic effects were prescribed (data not shown).
5 Conclusions
The efficacy and safety results of this every day, clinical practice study support the development of perindopril/indapamide/amlodipine in a single-pill fixed-dose tripledrug formulation. Although this trial was not designed to evaluate long-term outcomes, extensive clinical data describing these drugs as monotherapies and dual therapies suggest that the impact of treatment with this triple combination on morbi-mortality rates would be significant.
Şəkillər
Açar sözlər
İstinadlar
1. Lewington S,ClarkeR,QizilbashN,Peto R, CollinsR.Age-specific relevance of usual bloodpressure to vascular mortality:a meta-analysis of individual data for one million adults in 61prospective studies. Lancet. 2002;360(9349):1903–13.
2. Adler AI, Stratton IM,Neil HA,Yudkin JS, Matthews DR, Cull CA, etal. Association of systolic bloodpressure with macro-vascular and microvascular complications oft ype 2 diabetes (UKPDS36): prospective observational study. BMJ.2000;321(7258):412–9.
3. Chobanian AV, Bakris GL, BlackHR, Cushman WC, Green LA,Izzo JLJr, etal.The Seventh Report of the Joint National Committee on prevention, detection, evaluation, and treatment of high bloodpressure: the JNC7 report. JAMA.2003;289(19):2560–72.
4. Jackson JH, Sobolski J, Krienke R, Wong KS, Frech-Tamas F, Nightengale B. Bloodpressure control and pharmaco therapy patterns in the United States before and after there lease of the Joint National Committee on the prevention,detection, evaluation, and treatment of highbloodpressure(JNC7) guidelines. JAm Board FamMed.2008;21(6):512–21.doi:10.3122/jabfm.2008.06.080025.
5. Thoenes M,Neuberger HR,Volpe M, Khan BV, Kirch W, Bohm M. Antihypertensive drug therapy and bloodpressure control in men and women: aninternational perspective. JHum Hypertens. 2010;24(5):336–44.doi:10.1038/jhh.2009.76.
6. Bramlage P, Bohm M,Volpe M, Khan BV, Paar WD,Tebbe U,etal. A global perspective on bloodpressure treatment and control in are ferredcohortof hypertensive patients. J Clin Hypertens(Greenwich). 2010;12(9):666–77.doi:10.1111/j.1751-7176.2010.00322.x.
7. Law MR,Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with bloodpressure lowering drugs: ana-lysis of 354randomised trials. BMJ.2003;326(7404):1427.
8. Egan BM,Bandyopadhyay D,Shaftman SR,Wagner CS, Zhao Y,Yu-Isenberg KS. Initialmono therapy and combination therapy and hypertension contro lthe first year. Hypertension.2012;59(6):112431. doi:10.1161/HYPERTENSIONAHA.112.
194167.
9. Mancia G,Fagard R, Narkiewicz K, Redon J,Zanchetti A, Bohm Metal. 2013ESH/ESC Guidelines for the management of arterial hypertension. BloodPress.2013.doi:10.3109/08037051.2013.812549.
10. National Clinical Guideline Centre. Hypertension. Clinical management of primary hypertension in adults (NICEclinical guideline127). London,United Kingdom 2011.
11. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, etal .2007 Guidelines for the management of arterial hypertension:The task force for the management of arterial hypertension of the European Society of Hypertension(ESH) and of the European Societyof Cardiology(ESC). J Hypertens.2007;25(6):1105–87.
12. Beckett NS, Peters R,Fletcher AE, Staessen JA, Liu L, Dumi- trascu D, etal.Treatment of hypertension in patients 80 years of age or older. NE ngl JMed.2008;358(18):1887–98.
13. Dahlo¨f B,Gosse P,GueretP, Dubourg O, de Simone G, Schmieder R, etal. Perindopril/indapamide combination more effective than enalapril in reducing bloodpressure and left ventricular mass: the PICXEL study. J Hypertens. 2005;23(11):2063–70.
14. Dahlo¨fB, Sever PS,Poulter NR,Wede lH, Beevers DG, Caulfield M, etal. Prevention of cardiovascul are vents with anantihyper-tensive regimen of amlodipineadding perindoprilas required versus atenololadding bendroflumethiazideasrequired,in the Anglo-Scandinavian Cardiac OutcomesTrial-Blood Pressure Lowering Arm(ASCOT-BPLA):amulticen trerandomisedcon-trolledtrial. Lancet.2005;366(9489):895–906.
15. Deanfield JE, Detry JM, Lichtlen PR, Magnani B, Sellier P,Thaulow E. Amlodipinereducestransientmyo cardial ischemiain patients with coronary artery disease:double-blind Circadian Anti-Ischemia Programin Europe(CAPETrial). JAm Coll Cardiol.1994;24(6):1460–7.
16. Fox KM. Efficacy of perindoprilinreduction of cardiovascular events among patients withs table coronary artery disease: ran-domised,double-blind, placebo-controlled,multicentretrial (the EUROPAstudy). Lancet.2003;362(9386):782–8.
17. Mogensen CE, Viberti G,Halimi S, Ritz E, RuilopeL, Jermendy G, etal. Effectoflow-doseperindopril/indapamideon albumin-uriaindiabetes:preteraxinalbuminuriaregression:PREMIER.Hypertension.2003;41(5):1063–71.
18. Patel A, Mac Mahon S,Chalmers J, Neal B, Woodward M, Billot L, etal. Effects of afixed combination of perindopril and indapamideon macro vascular and microvascular out comes in patients with type 2 diabetes mellitus(theADVANCEtrial):a randomisedcontrolledtrial.Lancet.2007;370(9590):829–40.
19. PROGRESS Collaborative group. Randomised trialofaperin-dopril-based bloodpressure-lowering regimen among 6,105 individuals with previous strokeor transientischaemic attack. Lancet.2001;358(9287):1033–41.
20. van Vark LC, Bertrand M,Akkerhuis K M, Brugts JJ, Fox K,
Mourad JJ, etal. Angiotensin-convertingenzyme inhibitors reduce mortality in hypertension: ameta-analysis of randomized clinical trialsofrenin-angiotensin-aldosterone system inhibitors involving158,998patients. EurHeartJ.2012;33(16):2088–97.doi:10.1093/eurheartj/ehs075.
21. Chalmers J, Arima H, Woodward M,Poulter N, Mancia G, editors. Effects of combination of perindopril, indapamide and calcium channel blockers on deat hand cardiovascular out comes in patients with type2 diabetes in the ADVANCE trial (Abstract).23rdscientificmeetingoftheEuropeanSocietyofHypertension,Milan,Italy;2013.
22.PallD.The anti hypertensive efficacy of the perindopril-amlodipine-
indapamide combination. J Hypertens. 2012;30 (SupplA): e503.
23. KissI. A hypertoniabetegse´gfeln} ottkorie´sgyermekkorike-zele´se´nekszakmaie´sszervezetiira´nyelvei. Hypertoniae´s Nephrologia.2009;13: 81–168.
24. Weber MA, Julius S, Kjeldsen SE, Brunner HR, Ekman S, Hansson L, etal. Bloodpressure dependent and independent effects of antihypertensive treatment on clinical events in the VALUETrial. Lancet.2004;363(9426):2049–51.
25. Kikuya M, Hozawa A, Ohokubo T, TsujiI, Michimata M, Matsubara M, etal. Prognostic significance of bloodpressure and heart rate variabilities: the Ohasama study. Hypertension.2000;36(5):901–6.
26. Ceconi C, Fox KM, Remme WJ, Simoons ML, Bertrand M, Parrinello G,etal.ACE inhibition with perindopril and endo-thelialfunction. Results of asub study of the EUROPA study: PERTINENT. Cardiovasc Res.2007;73(1):237–46.
27. Koz C, Baysan O,Yokusoglu M, Uzun M,Yildirim M, Hasimi A, etal.Thee ffects of perindoprilon aorti celasticityandinflam-matory markers in hypertensive patients. Med Sci Monit. 2009;15(7):PI41–5869690 [pii].
28. Asmar RG, London GM, O’Rourke ME, Safar ME. Improvement in bloodpressure, arterial stiffness and wave reflections with a very-low-doseperindopril/indapamide combination in hyperten-sive patient: acomparison with atenolol. Hypertension.2001;38(4):922–6.
29. Ghiadoni L,Magagna A, Kardasz I, Taddei S, Salvetti A. Fixed dose combination of perindopril andi ndapamide improves peripheral vascular function in essential hypertensive patients. Am JHypertens. 2009;22(5):506–12.oi:10.1038/ajh.2009.31.
30. Williams B, Lacy PS,Thom SM, Cruickshank K, Stanton A, Collier D, etal. Differential impact of bloodpressure-lower ing drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation(CAFE) study. Circulation. 2006;113(9):1213–25. doi:10.1161/CIRCULATIONAHA.105.
595496.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 23.Aug.2014
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 2187