

Abstract
The advent of drug-eluting stent (DES) technology for the treatmentofcoronary artery disease (CAD) has significantly reduced the problem of in-stent restenosis caused by neointimal hyperplasia. Some of the limitations of DES include treatment of small vessel disease, issues related to the duration of dual antiplatelet therapy (DAPT), and treatment failure leading to restenosis and late or very late stent thrombosis, especially in complex lesions subsets such as bifurcation lesions. In this light, drug-coated balloons (DCBs) represent an innovation with a high potential impact on the treatment of patients with CAD.
Full article
In this review, I want discuss the potential role of DCBs in the management of different subsets of native CAD, and I will review the literature on this interesting topic and increasing field of application.
Bifurcation Lesions
Bifurcation lesions represent a constant challenge in the Cath Lab. Several technologies such as dedicated bifurcation stents were attempted in this subset of lesions, with contrasting results. The potential advantages on the use of a DCB in bifurcations are:
Homogeneous administration of the drug, whereas the DES only delivers the drug in the proximity of the struts. Delivery of high concentrations of drug into the vessel wall at the moment of injury. Respecting the original anatomy of the carina of the bifurcation
Avoidance of crushing of polymersandun controlled drug release (in case of two DES)
Potential decrease in DAPT with potentially reduced risk of very late thrombosis due to the absence of polymers
The first study that aimed at assessing the potential role of DCB for bifurcation lesions was the PEPCAD V registry, a prospective, multicenter single-arm trial that enrolled 28 patients with coronary bifurcation lesions treated with sequential first-generation DCB (SeQuent Please, B. Braun, Germany) inflation in both branches followed by bare-metal stent (BMS) implantation in the main branch (MB) alone (four patients received bailout stenting of SB). Nine-month angio- graphic follow-up showed a rate of binary restenosis of 3.8% and 7.7% in the MB and side branch (SB), respectively. Late lumen loss (LLL) was 0.38 ± 0.46 mm in the MB and 0.21 ± 0.48 mm in the SB. Three patients had SB restenosis, of which only one underwent TLR. There were also two episodes of ST. This study proved the feasibility of DCB use in the SB of complex bifurcation coronary lesions; how- ever the limited population enrolled, the lack of a control group, and the inadequate lesion preparation before DCB use were its major drawbacks.
Later, the DEBIUT study randomized 120 patients to three different strategies: 40 patients received a dilatation of both branches with DCB (Dior I generation, Eurocor, Germany) followed by BMS implantation in the MB, 37 patients received a predilatation of both branches with a semicompliant balloon followed by BMS implantation in the MB, and 40 patients received a predilatation of both branches with a semicompliant balloon followed by paclitaxel-eluting stent implantation. At 6-month angiographic follow-up, LLL was not significantly different in the BMS and DCB + BMS groups (0.49 vs. 0.41, p = NS), while DES treatment was associ- ated with a superior angiographic outcome (LLL 0.19 mm, p = 0.001 vs. both the other treatment allocations). Twelve-month clinical follow-up showed a similar rate of MACE (20%, 29.7%, and 17.5%, respectively; p = 0.40 for all comparisons); however the study was not powered enough to detect a clinical difference among treatments. The results of the DEBIUT study that tested a BMS + DCB strategy for SB treatment showed that this association does not warrant any advantage over a DES strategy, with a lower angiographic performance.
The BABILON trial was a multicenter study that randomized patients with bifurcation lesions, to MB and SB through sequential dilation with the SeQuent Please DCB (56 patients), or DES implantation in the MB and provisional SB stenting with T-stent technique (56 patients) after predilatation of both branches. Dual antiplatelet treatment was prescribed for 3 and 12 months, respectively. This study enrolled patients with complex bifurcation lesions, with type 1,1,1 Medina lesions being 57.4% overall. The final kissing balloon inflation rate was 15.7% in the DCB and 35.7% in the DES group (p = 0.019). SB bailout stenting was, respectively, 7.8% vs. 8.9% (p = 1). The primary endpoint, in-segment LLL at 9-month angiographic follow-up, adjudicated in 86 patients, was 0.31 ± 0.48 and 0.16 ± 0.38, respectively (p = 0.15). Side branch LLL was, respectively, 0.04 ± 0.76 and 0.03 ± 0.51 (p = 0.98). After the 24-month clinical follow-up, the two strategies were found safe, with no casualties registered. On the other hand, the co-primary endpoint, the rate of 24-month MACE, and the secondary endpoint of TLR were higher in the DCB group (17.3% vs. 7.1% (p = 0.105) and 15.4% vs. 3.6% (p = 0.045)). Interestingly, MB restenosis was signifi- cantly higher in the DCB group (13.5% vs. 1.8%; p = 0.027), but SB restenosis was similar in the two treatments (5.8% vs. 3.6%, p = 0.67). The main information that can be summarized from this study is that the DCB tested was inferior to DES when used in medium- to large-caliber MB vessels, with a high safety and efficacy profile when used in the SB, where LLL and TLR were low and similar to the other strategy tested.
The BIOLUX-I study was a prospective, single-arm multicenter study which investigated the efficacy of the Pantera Lux (Biotronik AG, Switzerland) DCB for SB treatment only. The 35 patients enrolled received direct SB treatment with DCB, followed by MB-DES implantation. Nine-month angiographic and intravascular ultrasound follow-up showed a SB LLL of 0.10 ± 0.43 mm (primary endpoint) with no cases of binary restenosis. Twelve-month clinical follow-up showed a total rate of MACE of 5.9%, with a rate of TLR of 2.9% and no stent thrombosis.
Recently, the DEBSIDE study analyzed the treatment of 50 patients treated with DES in the MB (Nile PAX) and DCB on the SB (Danubio DCB, Mynvasis, France). The 6-month angiographic follow-up showed a SB LLL of −0.04 ± 0.33, with a MLD of 1.55 ± 0.35 mm. At the clinical follow-up of 12 months, the inci- dence of TLR in the MB and SB was 10% and 2%, respectively.
Another study named SARPEDON assessed the role of DCB for SB ostium treatment after DES implantation in the MB followed by kissing balloon inflation. Angiographic follow-up showed a LLL of MV and SB of 0.21 ± 0.35 mm and 0.09 ± 0.21 mm respectively, with a restenosis rate of 4.0% and 6.0% (interestingly, in all cases SB restenosis involved the ostium). One-year clinical follow-up showed a rate of MACE of 19%, including three TVR and two deaths.
The Italian Interventional Cardiology Society (SICI-GISE) position paper gives an indication of Class IIb level of evidence C for the use of DCB plus BMS implanta- tion in the MB. Moreover, DCB dilatation in both branches is suggested as safe and effective, recommending the TAP technique (T stenting plus small protrusion) in case of SB stenting. The German consensus group recommends the use of DCB alone after predilatation of both branches and final satisfactory result. In case of need for stent implantation (e.g., for residual major dissection after predilatation), the association of DCB plus BMS is indicated as a valid alternative to traditional DES implantation in the MB
Small Vessel Disease
In the PICCOLETO randomized clinical trial, patients with stable or unstable angina undergoing PCI of small coronary vessels (2.75 mm or less) were randomized to Dior DCB (28 patients) or Taxus DES (Boston Scientific, USA) (29 patients). The primary study endpoint was percent diameter stenosis at 6-month angiographic follow-up (non-inferiority), and secondary endpoints were angiographic binary restenosis and occurrence of major adverse cardiac events (MACE: death, Q-wave myocardial infarction, TLR) at 9-month clinical follow-up. The two groups were not dissimilar regarding clinical and angiographic characteristics. Study was interrupted after enrolment of two-thirds of patients due to a clear superiority of the DES group. The primary endpoint was not met, because the PCB group showed a worse primary endpoint-higher percent diameter stenosis (43.6% vs. 24.3%, p = 0.029); angio- graphic restenosis was higher as well (32.1 vs. 10.3%, p = 0.043), whereas MACE were 35.7% in the PCB group and 13.8% in the DES group (p = 0.054). In this study, the Dior PCB failed to show a supposed equivalence to Taxus DES regarding angio- graphic endpoints during PCI of small coronary arteries. It was assumed that the lack of efficacy of the device used (which has since been retrieved from the marked for reduced efficacy, and later replaced by its second generation) rather than a class- effect in native coronary vessels. Moreover, we understood clearly how the predilata- tion of the lesion was crucial before DCB-PCI
In the SCAAR registry, which was an Internet-based registry from April 2009 to September 2011, 1129 patients were treated with paclitaxel-eluting balloons in Sweden. Mean follow-up was 328 ± 210 days. Nine hundred and nineteen patients were treated with a balloon using a contrast agent as a drug carrier (SeQuent Please, B. Braun, Germany) and 217 with a balloon without a drug carrier (Elutax first gen- eration, Aachen Resonance, Germany). The indications were predominantly de novo (45.4%) or in-stent restenotic (51.8%) lesions. The overall incidence of restenosis at 6 months was 3.4% with the DCB using a contrast agent as carrier, compared with 12.5% with the DCB without a carrier (risk ratio: 0.42; 95% confidence interval [CI] [0.26–0.68]). After adjusting for indications, lesion types, and procedural factors, the risk ratio was 0.39; 95% CI (0.24–0.65). This observational study from a large real- world population shows a major difference between two paclitaxel-eluting balloons. The findings suggest that there are no class effects for drug-eluting balloons and fac- tors other than the drug may be important for the clinical effect.
There is a number of registries showing low event rates with DCB-only angio- plasty in small vessel disease. The Paclitaxel-Eluting PTCA-Balloon Catheter to Treat Small Vessel (PEPCAD I) study (82 patients with 2.25–2.80 mm vessel diameter treated with SeQuent Please, PACCOCATH technology) showed a MACE rate (composite of death, MI, target lesion revascularization [TLR], lesion/stent thrombosis) of 6.1% and a TLR rate of only 4.9% at 3-year follow-up.
Real-world data from all-comer registries show consistent efficacy and safety of DCB when used for the treatment of native vessel disease. Zeymer et al. in a real-world prospective registry of 479 patients with small vessel disease (≥2.0 mm, ≤2.75 mm) treated with DCB angioplasty (SeQuent Please) showed a TLR rate of only 3.6% at 9-month follow-up. There were no cardiac deaths or other safety issues.
In the SeQuent Please worldwide all-comer registry, the DCB-only group (390 patients) showed low event rates, including MIs 0.7%, cardiac death 1.0%, TVR 1.0%, and TLR 1.0% at 9-month follow-up.
Ho et al. reported a TLR of 4% at 9 months in a real-world registry of 320 Southeast Asian patients treated with SeQuent Please DCB (76% de novo disease, 54% small vessels, and 76% presented with acute coronary syndromes [ACS]).
The single-arm, prospective multicenter Valentines II trial (103 patients, treated with second-generation DIOR® DCB) showed a TLR rate of 2.9%, a TVR of 6.9% (including TLR), 1.0% MI, and 0.0% cardiac death at 7.5 months.
The Leipzig Prospective Drug-Eluting Balloon-Registry reported 76 patients treated with a DCB-only (SeQuent Please) for native coronary artery disease with no occurrence of TLR at 2 years. The incidence of MI was 3.9% with nine deaths (all-causes) during follow-up.
A few years ago, data from a randomized clinical study became available. The BELLO (Balloon Elution and Late Loss Optimization) trial which was a prospective, multicenter trial that randomized 182 patients with lesions located in small vessels (reference diameter 2.8 mm or less) to treatment with paclitaxel DCB (I.Pact Falcon) Invatec-Medtroinic, USA) (n = 90) or Taxus implantation (n = 92). The primary end- point hypothesized was the non-inferiority in terms of angiographic in-stent (in- balloon) late lumen loss considering a difference of 0.25 mm. Secondary endpoints were angiographic restenosis, TLR, MACE, death, myocardial infarction, and target vessel revascularization, at 6 months. Baseline characteristics were well matched, except for a smaller vessel size in the DCB group (2.15 ± 0.27 mm vs. 2.25 ± 0.24 mm; p = 0.003). Interestingly, the majority (89%) of lesions involved vessels with a diam- eter of <2.5 mm. Bailout stenting was required in 20% of the lesions in the DCB group. The primary endpoint of LLL resulted significantly lower with DCB compared with Taxus (0.08 ± 0.38 mm vs. 0.29 ± 0.44 mm); therefore the non-inferiority was met moreover, with a demonstrated superiority of the DCB over the DES arm. At 6 months, DCB and DES were associated with similar rates of angiographic resteno- sis (8.9% vs. 14.1%; p = 0.25), target lesion revascularization (4.4% vs. 7.6%; p = 0.37), and MACE (7.8% vs. 13.2%; p = 0.77). The authors of the study concluded that treatment of small vessel disease with a paclitaxel DCB was associated with less angiographic late loss and similar rates of restenosis and revascularization compared to a PES . Even more interesting, the extended follow-up suggested that the treat- ment of small vessels with DCB had an improved efficacy compared with PES treat- ment at 3-year follow-up in support of the 1-year observation: a statistically significant benefit with regard to MACE at 3 years with DCB when compared with PES was shown (Fig 1).
Between 2012 and 2015, all patients treated with Elutax SV DCB (Aachen Resonance, Germany) at nine Italian centers were enrolled in a retrospective registry. Primary outcome was the occurrence of target lesion revascularization (TLR) at the longest available follow-up. Secondary endpoints were procedural success and the occurrence of device-oriented adverse cardiovascular events including cardiac death, target vessel myocardial infarction, stroke, and TLR. A minimum 6-month clinical follow-up was required to enter the study. The study enrolled 544 consecutive patients treated for 583 coronary lesions, 53% having ISR and 47% native vessel disease. Procedural success was high and occurred in 97.5% of the entire population. At the longest available clinical follow-up, with an of average 13.3 ± 7.4 months, 5.9% of the patients suffered a TLR and 7.1% a device-oriented adverse cardiovas- cular event. A subanalysis of the data comparing patients treated for ISR and patients treated for de novo lesions showed a consistent and significant difference in the TLR rate which occurred in 9% of the ISR vs. 2.6% of the native vessels (p = 0.006); device-oriented adverse cardiovascular events (DOCE) were significantly higher in the ISR group as well (11 vs. 2.6%; p = 0.001), whereas no significant statistical difference was observed in terms of cardiac death, TV-MI, and stroke. This registry on the performance of a new-generation DCB showed an adequate profile in terms of safety and efficacy at mid-term clinical follow-up. This real-world, all-comer registry also showed, as other studies with different devices had previously shown, how the use of DCB in native vessels is safe and more effective than in the ISR setting.
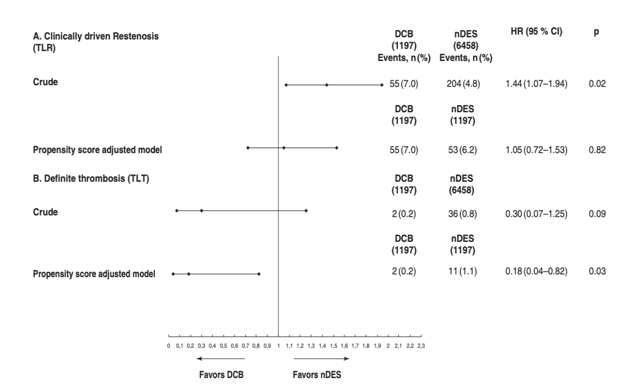
Another piece in the puzzle derives from the recently just-published post hoc analysis of the SCAAR registry. Authors analyzed all DCB or new-generation DES used for the treatment of de novo coronary lesions between 2009 and 2016, for a total of 1197 DCB and 6458 DES implanted. TLR and definite target lesion throm- bosis (TLT) were evaluated as co-primary study endpoints, with a median follow-up of 901 days. DCB patients were older, with higher cardiovascular risk profile. Bailout stenting after DCB was performed in 8% of the caseslesions, according to the suggested indications from Consensus Documents. The cumulative rate of TLR and TLT was 7.0% vs. 4.9% and 0.2% vs. 0.8% for DCB and DES, respectively. Before adjustment, DCB was associated with a higher risk of TLR [hazard ratio (HR) 1.44; 95% confidence interval (CI) 1.07 – 1.94] and a nonsignificantly lower risk of TLT (HR 0.30; 95% CI 0.07 – 1.24), which was modified after the use of a propensity-matched model. The final population consisted of 1197 DCB- and 1197 DES-treated patients, and treatment with DCB was associated with a similar risk for TLR (adjusted HR 1.05; 95% CI 0.72 – 1.53) but a significantly lower risk for TLT (adjusted HR 0.18; 95% CI 0.04 – 0.82) compared to DES (Fig 2) The study concluded that the treatment with DCB for native vessels was safe and effective, at least as with current generation DES. Therefore, in selected cases, DCB appears as a good alternative to DES (Table 1).
ST Segment Elevation Myocardial Infarction
Another potentially interesting application of DCB could be the management of a selected population of patients suffering acute ST-elevation myocardial infarction (STEMI). First results of the DEB-AMI (drug-eluting balloon in acute STEMI) trial showed that DCB followed by BMS implantation failed to show angiographic superiority versus a strategy of BMS only, and angiographic results of DES were superior to both BMS and DCB.
Later, the non-randomized fourth arm of the DEB-AMI trial was published. This additional study aimed to compare a DCB-only strategy with the three other treat- ments evaluated in the aforementioned study. This arm yielded an angiographic outcome comparable to BMS alone and DCB followed by BMS. Therefore, the authors considered a DCB-only strategy to be a potential treatment alternative dur- ing primary PCI in patients with contraindications to DES . This study was done with the first generation of the Dior balloon that had already shown to be ineffective in delivering a proper dose of paclitaxel to the vessel wall.
Although the aforementioned trials could not prove that DCB only was equivalent to DES, the ongoing prospective, single-center randomized REVELATION trial study will shed light on this thematic. This study will randomize 120 patients to DCB or DES, and primary endpoint will be lesion assessment with fractional flow reserve after 9 months during angiographic follow-up, with a cutoff of 0.90 (non- inferiority attested at 0.85) decided by the investigators to determine the potential equivalence of the 2 strategies. All patients will be followed up clinically for 5 years.
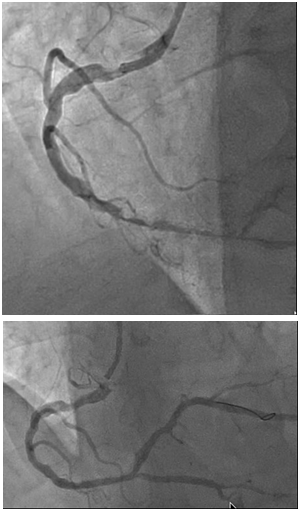
In view of delayed healing and endothelial dysfunction induced by DES and the concept that local drug delivery to the culprit plaque at the moment of highest inflam- mation, DCB seems still to be an attractive treatment opportunity in STEMI patients. However, currently available data do not suggest their routine use in this setting. An interesting setting could be the management of STEMI caused by ISR, after proper lesion preparation with either manual thrombus aspiration or predilatation (Figs. 3, 4, 5 and 6.). In this setting, avoiding the implantation of a further stent when this strategy has just failed seems particularly appealing.
Do We Need Stents After DCB in Native Coronary Vessels?
Among the limitations reported for DCB use for de novo lesions is the rather high proportion of “bailout stenting,” usually caused by suboptimal angio- graphic results, such as dissection or impaired distal flow. However, all the studies analyzed have shown a very variable rate of stent use after DCB, ranging from 30% during the initial experiences to less than 10% in the current series. As already stated, we would like to underline how physicians should maintain the rate of stent implantation after DCB below 10%, in order to get the maximum from this technology. Type A and B, not flow-limiting dissec- tions, should not be treated with stenting and should be checked after 5–10 min in order to assess a possible worsening of the dissection or vessel recoil. If this event does not occur, this type of lesions should be left untreated, as we have previously shown.
In a prospective observational study whose aim was to investigate the outcome of a consecutive series of patients with native CAD treated with second-generation DCB and residual coronary dissection at two Italian centers where the clinical con- ditions were evaluated at 1 and 9 months, and angiographic follow-up was under- taken at 6 months, we observed the sealing of most of dissections without significant neointimal hyperplasia, with an angiographic outcome similar to the one of DCB left without dissection.
Recent Scientific Evidence on the Role of DCB for Native Vessel Disease
Recently, the BASKET-SMALL 2 trial was presented at the European Society of Cardiology (ESC) Conference in Munich (August 2018) and contemporarily pub- lished in The Lancet Journal. The scope of this trial was to assess the possible advantages of DCB in terms of: (1) favourable vascular remodeling, (2) avoidance of prosthesis implantation and (3) the option of shortening the duration of dual anti- platelet therapy in small vessel disease management. The BASKET SMALL 2 was a multicentre, open-label, randomized non-inferiority trial which enrolled 758 patients with de novo coronary lesions (diameter up to 3 mm). Patients were ran- domly allocated (1:1) to Sequent Please DCB or DES (25% Taxus and 75% Xience, Abbott Vascular, USA), after successful predilatation. The primary hypothesis of the trial was to demonstrate the non-inferiority of DCB (382) versus DES (376) in terms of MACE (cardiac death, non-fatal myocardial infarction and TVR) at 12 months. Non-inferiority of DCB versus DES was shown because the 95% CI of the absolute difference in MACE in the per-protocol population was below the predefined margin (–3.83 to 3.93%, p = 0.0217). After 12 months, the proportions of MACE were similar in both groups of the full-analysis population (7.5% for DCB vs. 7.3% for DES; HR 0.97 [95% CI 0.58–1.64], p = 0.9180). The other clinical endpoints (cardiac death, TVR and MI) were not dissimilar in the two populations. The study authors concluded that in small vessel disease, a current generation, effective DCB was non-inferior to the current genera- tion (at least, in 75% of the cases in this study!) DES in terms of hard clinical end- points. There are some limitations for this study, including the absence of core lab for basal lesion assessment, the short follow-up and the high experience of the oper- ators who participated in the study, which means that these results cannot be gener- alized to other less expert operators. Finally, these results were obtained with just one type of DCB and to this day we do not have data to suggest that a similar result can be extended to other devices. However, the results of the BASTEK SMALL II study are an important tool to assess the role of DCB for native coronary vessel treatment, and this should be considered a ground-breaking study in this field.
Figures
Keywords
References
1. Cortese B, Bertoletti A. Paclitaxel coated balloons for coronary artery interventions: a compre- hensive review of preclinical and clinical data. Int J Cardiol. 2012;161(1):4–12.
2. Belkacemi A, Agostoni P, Voskuil M, Stella PR. Coronary bifurcation lesions treated with the drug-eluting balloon: a preliminary insight from the DEBIUT study. EuroIntervention. 2011;7:K66–9.
3. Stella PR, Belkacemi A, Dubois C, et al. A multicenter randomized comparison of drug- eluting balloon plus bare-metal stent versus bare-metal stent versus drug-eluting stent in bifur- cation lesions treated with a single-stenting technique: six-month angiographic and 12-month clinical results of the drug-eluting balloon in bifurcations trial. Catheter Cardiovasc Interv. 2012;80(7):1138–46.
4. Schulz A, Hauschild T, Kleber FX. Treatment of coronary de novo bifurcation lesions with DCB only strategy. Clin Res Cardiol. 2014;103(6):451–6.
5. Mínguez L, Ramón J, Asensio N, Manuel J, Vecino D, Javier L, et al. A prospective randomised study of the paclitaxel-coated balloon catheter in bifurcated coronary lesions (BABILON trial): 24-month clinical and angiographic results. EuroIntervention. 2014;10(1):50–7.
6. Waksman R, Serra A, Loh JP, et al. Drug-coated balloons for de novo coronary lesions: results from the valentines II trial. EuroIntervention. 2013;9(5):613–9.
7. Worthley S, Hendriks R, Worthley M, et al. Paclitaxel-eluting balloon and everolimus-eluting stent for provisional stenting of coronary bifurcations: 12-month results of the multicenter BIOLUX-I study. Cardiovasc Revasc Med. 2015;16(7):413–7.
8. Berland J, Lefèvre T, Brenot P, Fajadet J. DANUBIO–a new drug-eluting balloon for the treat- ment of side branches in bifurcation lesions: six-month angiographic follow-up results of the DEBSIDE trial. EuroIntervention. 2015;11(8):868–76.
9. Jim M-H, Lee M K-y, Fung R C-y, et al. Six month angiographic result of supplementary paclitaxel-eluting balloon deployment to treat side branch ostium narrowing (SARPEDON). Int J Cardiol. 2015;187:594–7.
10. Cortese B, Berti S, Biondi-Zoccai G, et al. Drug-coated balloon treatment of coronary artery disease: a position paper of the Italian Society of Interventional Cardiology. Catheter Cardiovasc Interv. 2014;83(3):427–35.
Kleber FX, Mathey DG, Rittger H, et al. How to use the drug-eluting balloon: recommenda- tions by the German consensus group. EuroIntervention. 2011;7:K125–8.
11. Picard F, Doucet S, Asgar AW. Contemporary use of drug-coated balloons in coronary artery disease: where are we now? Arch Cardiovasc Dis. 2017;110(4):259–72.
12. Cortese B. The PICCOLETO study and beyond. EuroIntervention. 2011;7:K53–6.
13. Bondesson P, Lagerqvist B, James SK, et al. Comparison of two drug-eluting balloons: a report from the SCAAR registry. EuroIntervention. 2012;8(4):444–9.
Unverdorben M, Kleber FX, Heuer H, et al. Treatment of small coronary arteries with a paclitaxel-coated balloon catheter in the PEPCAD I study: are lesions clinically stable from 12 to 36 months? EuroIntervention. 2013;9(5):620–8.
14. Zeymer U, Waliszewski M, Spiecker M, et al. Prospective ‘real world’ registry for the use of the ‘PCB only’ strategy in small vessel de novo lesions. Heart. 2013;100(4):311–6.
15. Cortese B, Fetiveau R, Carrera A, et al. TCT-417 treatment of coronary artery disease with a new-generation drug-coated balloon: preliminary results from the Italian Elutax SV registry. J Am Coll Cardiol. 2015;15(66):B169–70.
16. Teo LYL, Khurana R, Jafary FH, Ooi YW. Clinical efficacy and safety of sequent please paclitaxel-eluting balloon in a real-world multi-center registry of south-east Asian patients. Am J Cardiol. 2013;111(7):28B.
17. Uhlemann M, Möbius-Winkler S, Adam J, et al. The Leipzig prospective drug-eluting balloon- registry—outcome of 484 consecutive patients treated for coronary in-stent restenosis and De novo lesions using paclitaxel-coated balloons. Circ J. 2016;80(2):379–86.
18. Latib A, Colombo A, Castriota F, et al. A randomized multicenter study comparing a paclitaxel drug-eluting balloon with a paclitaxel-eluting stent in small coronary vessels: the BELLO (bal- loon elution and late loss optimization) study. J Am Coll Cardiol. 2012;60(24):2473–80.
19. Latib A, Ruparelia N, Menozzi A, et al. 3-year follow-up of the balloon elution and late loss optimization study (BELLO). J Am Coll Cardiol Interv. 2015;8(8):1132–4.
20. Richelsen RKB, Overvad TF, Jensen SE. Drug-eluting balloons in the treatment of coronary De novo lesions: a comprehensive review. Cardiol Ther. 2016;5(2):133–60.
21. Cortese B, D’Ascenzo F, Fetiveau R, et al. Treatment of coronary artery disease with a new- generation drug-coated balloon: final results of the Italian Elutax SV rEgistry-DCB-RISE. J Cardiovasc Med (Hagerstown). 2018;19(5):247–52.
22. Giannini F, Naim C, Costopoulos C, et al. Drug-coated balloons in interventional cardiology. Expert Rev Cardiovasc Ther. 2013;11(10):1379–91.
Belkacemi A, Agostoni P, Nathoe HM, et al. First results of the DEB-AMI (drug elut- ing balloon in acute ST-segment elevation myocardial infarction) trial. J Am Coll Cardiol. 2012;59(25):2327–37.
23. Nijhoff F, Agostoni P, Belkacemi A, et al. Primary percutaneous coronary intervention by drug-eluting balloon angioplasty: the nonrandomized fourth arm of the DEB-AMI (drug- eluting balloon in ST-segment elevation myocardial infarction) trial. Catheter Cardiovasc Interv. 2015;86(S1):S34–44.
24. Vos NS, van der Schaaf RJ, Amoroso G, et al. REVascularization with paclitaxEL-coated bal- loon angioplasty versus drug-eluting stenting in acute myocardial infarcTION—A randomized controlled trial: rationale and design of the REVELATION trial. Catheter Cardiovasc Interv. 2016;87(7):1213–21.
25. Gao L, Chen Y-D. Application of drug-coated balloon in coronary artery intervention: chal- lenges and opportunities. J Geriatr Cardiol. 2016;13(11):906–13.
26. Waksman R, Pakala R. Drug-eluting balloon: the comeback kid? Circ Cardiovasc Interv. 2009;2(4):352–8.
27. Calé R, Sousa PJ, Pereira E, et al. One-year clinical outcomes of percutaneous treatment with drug-eluting balloons: results from a multicenter registry. Rev Port Cardiol. 2013;32(5):361–9.
28. Maier LS, Maack C, Ritter O, Böhm M. Hotline update of clinical trials and registries pre- sented at the German Cardiac Society meeting 2008. (PEPCAD, LokalTax, INH, German ablation registry, German device registry, DES.DE registry, DHR, reality, SWEETHEART registry, ADMA, GERSHWIN). Clin Res Cardiol. 2008;97(6):356–63.
29. Xiu PY, Meier P. What are the barriers to the use of drug-eluting balloons? Interv Cardiol. 2014;6(1):9.
30. Cortese B, Silva Orrego P, Agostoni P, et al. Effect of drug-coated balloons in native coronary artery disease left with a dissection. J Am Coll Cardiol Intv. 2015;8(15):2003–9.
31. Wickramarachchi U, Eccleshall S. Drug-coated balloon-only angioplasty for native coronary disease instead of stents. Interv Cardiol Rev. 2016;11(2):110–5.
32. Raban V, Ahmed F, Ohlow MA, et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): an open-label randomised non-inferiority trial. Lancet. 2018;6736(18):31719–7. Daxil olub 14.10.2023
Article Info:
Publication history
Published: 29.Dec.2023
Copyright
© 2013-2025. Azerbaijan Society of Cardiology. Published by "Uptodate in Medicine" health sciences publishing. All rights reserved.Related Articles
Viewed: 2180