

Abstract
Aortic regurgitation (AR) prevalence increases with age, when patient present AR relateted symptoms, then prognosis is poor. Transcatheter aortic valve implantation for patients with pure severe AR and at high surgical risk is occasionally performed, but remains a clinical challenge due to absence of valvular calcium, large aortic root and increased stroke volume. In standarad TAVI for AS , the presence of aortic annular calcification acts as a landmark for positioning and stabilization during deployment.These issues make the positioning and deployment of transcatheter aortic valve implantation devices unpredictable, with a tendency to prosthesis embolisation or malposition. Our patient with aortic insufficiency, who presented with cardiogenic shock, could not be operated due to high surgical risk and accepted all the mentioned complications, it was decided to perform TAVI. After 5 days, our patient's condition was completely stabilized and sent home, due to we present this case.
Full article
Clinical Case: A 72-year-old woman with a past medical history of chronic kidney disease,diabetes mellitus and recurrent pulmonary edema was admitted to the intensive care unit with cardiogenic shock after 15 day hospitalitation in another hospital. Her vital signs show BP- 93/26 Hg with inotropic agents (noradrenalin, dobutamin), HR- 106 bpm, RR- 28 bpm, SPO2 96% on 9L oxygen, temperature 36.5-37 C. She was unresponsive, GCS 8. There were bibasilar crackles on lung auscultataion and a grade 4/6 decrescendo,blowing diastolic murmur was heard along the left sternal border on the precordial exam and bounding carotid pulse. She had a urinary catheter in place with adequate urine output 10 ml per hour with furosemid stimulation.
Analysis: Hb-8.7, Hct-26.0, WBC-12.74, RBC -3.28, creatinine- 2.03 mg/dl, lac-5, pro-BNP-3345, albumin 32.5g/l, CRP-42.67mg/l
ECG: Atrial fibrillation, left axis deviation
X-RAY: Enlarged cardiac siluette
Echocardiography was performed, which revealed severe aortic insufficiency, moderate MR, moderate TR, LVEF 45%
Cardiac CT : severe left ventricule and atrium dilatation (LV diametr- 62 mm, LA diametr 61 mm)
- the mean annular diameter-24.6mm,the perimeter of annulus 80.9mm, mean diameter of sinus Valsalva- 27.6 mm, ascending aorta -31mm
- RCA ostia height- 18.5 mm , LMCA ostia height-14 mm.
Clinical course. Patient condition was getting worse, although we increased inotropic agent doses, pressure was dropping, and urine output low. The case was discussed between cardiology and cardiosurgery team and current unstabil condition of the patient, the age, the surgical risk, and the absence of findings suggesting the need to intervene the aortic root, percutaneous management was chosen.
Coronary Angiography: LMCA-N, LAD mid 70%, Cx mid 90%, OM ostium 50%, RCA prox 60%
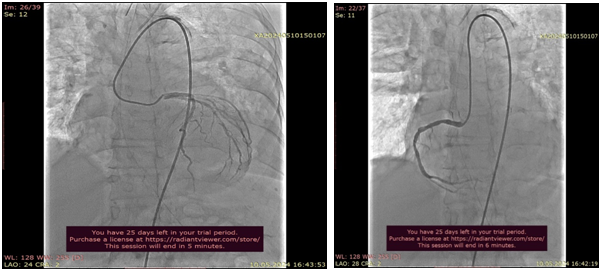
TAVİ: The procedure was performed under general anesthesia. A temporary pacemaker was implanted via left femoral vein. A pigtail catheter was placed in the noncoronary cusp, and a stiff Confida wire was placed inside the left ventricle. The 29 mm Medtronic Evolute Valve was carefully advanced until the aortic annulus, positioned and deployed under rapid ventricular pacing. The deployment was carried out in an extremly slow and careful, in a single attempt. After deployment,rapid ventricular pacing stimulation was kept. Hemodynamically significant leakage and gradient were not observed in the valve.
There was immediate improvment in hemodynamics following valve deployment.The diastolic pressure was 24 mmHg and it recovered to 58 mmHg immediately post-deployment. During 1h follow-up after procedure urine output was 150 ml/h. We stopped furosemid infusion and after that urine output was 100-150 ml/ per h.After 1 day inotrop support we stopped inotropic agents also and daily blod pressure interval 115-125/ 55-60 mmHg.
Postopertativ echocardiography: no PVL, moderate MR, moderate TR, LVEF 50%.
48 h after TAVI, intermittant AV block occured. In the period of AV block multiple complete AV block assosiated torsed des pointes episodes observed in the monitor. Temporarly pacemaker was placed immediatly and VT epiodes solved. After 24 h AV block solved . The patient improved clinically, her laboratory results in normal range and she was discharged home. During follow-up, the patient had considerable clinical improvement, with better quality of life and NHYA II
Conclusion: Menagement of this patient with severe aortic regurgitation and severe aortic regurgitation assosiated cardiogenic shock had a several prosedural challanges. This patient had no realistic chance to survive without this procedure. That is why there has been special interest in TAVI use patient who have pure aortic regurgitation and limited surgical approach. In this case we have excelent procedural outcome with no residual aortic regurgitation, and it is show that TAVI is lifesaving choice very high risk patient with severe pure aortic regurgitation.
Figures
Keywords
References
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8823702/
2. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)02806-4/abstract
3. https://www.sciencedirect.com/science/article/pii/S0019483216300013
Article Info:
Publication history
Published: 29.Oct.2024
Copyright
© 2013-2025. Azerbaijan Society of Cardiology. Published by "Uptodate in Medicine" health sciences publishing. All rights reserved.Related Articles
Viewed: 2922